The document reviews the management of high-risk cardiovascular conditions during pregnancy. It discusses the normal physiological changes in pregnancy, including increased blood volume and cardiac output. It emphasizes the importance of pre-conception counseling and risk stratification to discuss risks, medications, contraception and optimize cardiac status. Risk of complications is based on general factors like functional status and lesion-specific predictors. Conditions associated with high risk include severe valve disease, complex congenital heart disease, pulmonary hypertension, aortopathies and dilated cardiomyopathy. Close monitoring during pregnancy and delivery is recommended depending on the specific condition.
Risk factors of Acute Coronary Syndrome at Prince Ali Bin Alhussein hospitalMinistry of Health
Objective:The aim of this survey to identify the relationship between ACS and its risk factors and the association between the risks factors themselves. Method: A retrospective study depends on the registered files of the admitted patients to Prince Ali Bin Alhussein hospital with ACS since April 2013 till October of 2013 included 174 patients. Result:The above mentioned data and results show a strong relationship between ACS and the mentioned risk factors. Conclusion: There is a strong relationship between risks factors themselves as D.M and hypertension, and between hypertension with the sex and smoking.There's an association between D.M and the patient's gender
Risk factors of Acute Coronary Syndrome at Prince Ali Bin Alhussein hospitalMinistry of Health
Objective:The aim of this survey to identify the relationship between ACS and its risk factors and the association between the risks factors themselves. Method: A retrospective study depends on the registered files of the admitted patients to Prince Ali Bin Alhussein hospital with ACS since April 2013 till October of 2013 included 174 patients. Result:The above mentioned data and results show a strong relationship between ACS and the mentioned risk factors. Conclusion: There is a strong relationship between risks factors themselves as D.M and hypertension, and between hypertension with the sex and smoking.There's an association between D.M and the patient's gender
CORONARY ARTERY DISEASE IN WOMEN by DR ABHISHEK RATHOREdrabhishekbabbu
CAD is the leading cause of death in women. Here is the current scenerio of CAD in women. In what matter CAD in women differs from man is presented hare.
Maternal Cardiovascular Hemodynamics in Normal and Preeclamptic Pregnancies U...CrimsonPublishers-PRM
Maternal Cardiovascular Hemodynamics in Normal and Preeclamptic Pregnancies Using Echocardiography by Sonali S Somani in Perceptions in Reproductive Medicine_Crimson Publishers: Journal of Reproductive Health
CORONARY ARTERY DISEASE IN WOMEN by DR ABHISHEK RATHOREdrabhishekbabbu
CAD is the leading cause of death in women. Here is the current scenerio of CAD in women. In what matter CAD in women differs from man is presented hare.
Maternal Cardiovascular Hemodynamics in Normal and Preeclamptic Pregnancies U...CrimsonPublishers-PRM
Maternal Cardiovascular Hemodynamics in Normal and Preeclamptic Pregnancies Using Echocardiography by Sonali S Somani in Perceptions in Reproductive Medicine_Crimson Publishers: Journal of Reproductive Health
Stratified Management of Cardiac Surgery for Structural Heart Disease during ...semualkaira
We study pregnancy outcomes of cardiac surgery
under cardiopulmonary bypass (CPB) at different stages and discuss stratified management of cardiac surgery under CPB in pregnant women with structural heart disease (SHD) from pre-pregnancy counseling through postpartum management.
Stratified Management of Cardiac Surgery for Structural Heart Disease during ...semualkaira
: We study pregnancy outcomes of cardiac surgery
under cardiopulmonary bypass (CPB) at different stages and discuss stratified management of cardiac surgery under CPB in pregnant women with structural heart disease (SHD) from pre-pregnancy counseling through postpartum management.
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
2. contractions. Oxygen consumption increases 3-fold,
and systolic and diastolic BP rise during contractions.
Reduction of pain and apprehension with analgesia
and anesthesia may limit hemodynamic changes and
the rise in oxygen consumption. Cesarean delivery is
frequently recommended in women with cardiac
disease; however, it can be also associated with
considerable hemodynamic changes related to intu-
bation and drugs used for anesthesia. A temporary
increase in intracardiac pressures may occur imme-
diately after delivery due to relief of caval compres-
sion and blood shift from the contracting uterus into
the systemic circulation, which may lead to clinical
deterioration.
PREGNANCY RISK ASSESSMENT
Assessment of pregnancy risk is an important aspect of
the care of women with heart disease who are of
childbearing age (3). All women with cardiac disease
can benefit from pre-conception counseling, which
should include a detailed discussion of the risk of
pregnancy. Some women may require optimization of
cardiac status prior to pregnancy, and for those women
considering pregnancy, cardiac medications that are
teratogenic, such as warfarin and angiotensin-
converting enzyme inhibitors, can be switched to
safer medications when necessary. Increasing
numbers of women with heart disease are considering
fertility therapy, and in this circumstance, pre-
conception risk stratification and safety of fertility
therapy should be addressed. A discussion of safe
contraception choices is relevant for those who decide
not to become pregnant. It is important that this in-
formation is communicated effectively to patients; a
number of groups have shown that many women do
not fully understand pregnancy and contraception
risks (3–5).
Cardiologists with expertise in pregnancy and
heart disease should perform pre-conception coun-
seling and risk stratification. Issues to address at the
time of pre-conception counseling are shown in
Table 1. Risk assessment should include a complete
history and physical examination, a 12-lead electro-
cardiogram (ECG), and a transthoracic echocardio-
gram. In women who are pregnant, signs and
symptoms of pregnancy can mimic heart disease, and
should be interpreted accordingly. Risk stratification
may be further defined by incorporating other clinical
and imaging information, including disease activity,
cardiac computed tomography (CT), or cardiac mag-
netic resonance. Cardiac magnetic resonance and
CT findings should be reviewed and incorporated
into risk assessment, especially in women with
aortopathies and complex congenital lesions.
Exercise stress testing to measure functional
capacity and BP response to exercise is useful
for risk stratification in women with valve
lesions, such as aortic stenosis (AS) (6,7).
Cardiopulmonary testing, with measure-
ments of oxygen saturation, functional ca-
pacity, peak VO2, and chronotropic index,
provides helpful information in women with
complex CHD (8). Baseline and serial serum
B-type natriuretic peptide levels during
pregnancy can be incorporated into preg-
nancy assessment in women with the poten-
tial to develop heart failure (HF) during
pregnancy due to myocardial disease,
valvular heart disease, and CHD. In specific
cases, women with arrhythmias may benefit
from continuous ECG monitoring, exercise testing,
or electrophysiology studies. Women with inherited
cardiac conditions should have a formal genetic
evaluation to discuss transmission of disease to
offspring (6,9). Autosomal-dominant cardiac condi-
tions include Marfan, Noonan, William, Holt-Oram,
and 22q11 deletion syndromes, as well as some of
the inherited arrhythmias (long-QT syndrome) and
cardiomyopathies (hypertrophic cardiomyopathy).
Women with inherited cardiac conditions who have
an identified genetic mutation may wish to explore
the option of pre-implantation genetic screening.
Assessment with maternal fetal medicine specialists
(high-risk obstetricians) to discuss obstetric risk is an
important part of pre-conception assessment.
To estimate pregnancy risk, it is important to
consider general and lesion-specific risk predictors.
General risk predictors are relevant for all women
with heart disease and include factors such as cardiac
history, functional capacity, and ventricular function.
Lesion-specific risks are known for many, but not all,
cardiac conditions and are discussed later, in the
corresponding sections.
For women with pre-existing heart disease, the
most common cardiac complications during preg-
nancy are arrhythmias, HF, and thromboembolic
events (TEs). Early studies on pregnancy risk pre-
dictors identified functional class and cyanosis as
important determinants of adverse outcomes during
pregnancy (10–12). Subsequently, large pregnancy
cohorts were assembled, and pregnancy risk indexes
were developed (13–19), which are shown in Table 2.
The first prospective risk index was developed by the
CARPREG (Cardiac Disease in Pregnancy) in-
vestigators. The CARPREG study examined outcomes
in women with congenital and acquired heart disease
and identified 4 predictors of adverse maternal
A B B R E V I A T I O N S
A N D A C R O N Y M S
AC = anticoagulation
BPHV = bioprosthetic heart
valve
CHD = congenital heart disease
HF = heart failure
LMWH = low molecular weight
heparin
MPHV = mechanical prosthetic
heart valve
PHV = prosthetic heart valve
SCAD = spontaneous coronary
artery disease
TT = thrombolytic therapy
UFH = unfractionated heparin
J A C C V O L . 6 8 , N O . 4 , 2 0 1 6 Elkayam et al.
J U L Y 2 6 , 2 0 1 6 : 3 9 6 – 4 1 0 Pregnancy and Heart Disease: Part I
397
3. events: prior cardiac events; poor functional status
(New York Heart Association [NYHA] functional class
>II) or cyanosis; left heart obstruction; and systemic
(subaortic) ventricular systolic dysfunction (14). The
BACH (Boston Adult Congenital Heart) group studied
predictors of outcomes in women with congenital
heart disease and, in addition to the CARPREG risk
factors, identified smoking history and reduced sub-
pulmonary ventricular function and/or severe pul-
monic regurgitation as important determinants of
adverse outcomes during pregnancy (16). The
ZAHARA (Zwangerschap bij vrouwen met een Aan-
geboren HARtAfwijking-II [translated as “Pregnancy
in women with CHD II risk index”]) risk score was on
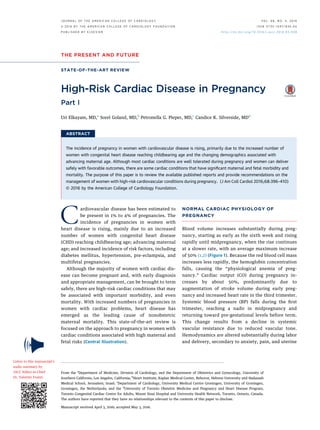
CENTRAL ILLUSTRATION High-Risk Heart Disease in Pregnancy
Pre-conception counseling and pregnancy risk stratification for all women with HRHD of childbearing age
In women considering pregnancy: Switch to safer cardiac medications and emphasize importance of close monitoring
In women avoiding pregnancy: Discuss safe and effective contraception choices or termination in early pregnancy
Valve disease
Complex congenital
heart disease
Pulmonary
hypertension Aortopathy
Dilated
cardiomyopathy
Pregnancy not advised
in women with:
• Severe mitral and aortic
valve disease
• Mechanical prosthetic
valves if effective
anticoagulation not
possible
Pregnancy not advised
in women with:
• Significant ventricular
dysfunction
• Severe atrioventricular
valve dysfunction
• Failing Fontan circulation
• O2
saturation <85%
Pregnancy not advised for:
• All women with
established pulmonary
arterial hypertension
Pregnancy not advised
in some women with:
• Marfan syndrome (MFS)
• Bicuspid aortic valve (BAV)
• Turner syndrome
• Rapid growth of aortic
diameter or family history
of premature aortic
dissection
Pregnancy not advised
in women with:
• Left ventricular ejection
fraction <40%
• History of peripartum
cardiomyopathy
Pregnancy management:
• Close follow-up
• Drug therapy for heart
failure or arrhythmias
• Balloon valvuloplasty or
surgical valve replacement
in refractory cases
Pregnancy management:
• Close follow-up
Pregnancy management:
• Close follow-up
• Early institution of
pulmonary vasodilators
Pregnancy management:
• Treat hypertension
• Beta-blockers to reduce
heart rate
• Frequent echo assessment
• Surgery during pregnancy
or after C-section if large
increase in aortic dimension
Pregnancy management:
• Close follow-up
• Beta-blockers
• Diuretic agents
for volume overload
• Vasodilators for
hemodynamic and
symptomatic improvement
Delivery:
• Vaginal delivery preferred
• C-section in case of fetal
or maternal instability
• Early delivery for clinical
and hemodynamic
deterioration
• Consider hemodynamic
monitoring during labor
and delivery
Delivery:
• Vaginal delivery preferred
• C-section in case of fetal
or maternal instability
• Consider hemodynamic
monitoring during labor
and delivery
Delivery:
• Vaginal delivery preferred
• C-section in case of fetal
or maternal instability
• Timing of delivery depends
on clinical condition and
right ventricular function
• Early delivery advisable
• Diuresis after delivery to
prevent RV volume overload
• Extended hospital stay
after delivery
Delivery:
• C-section in cases of
significant aortic dilation
MFS >40 mm
BAV >45 mm
Turner: ASI >20 mm/m2
Delivery:
• Vaginal delivery preferred
• C-section in case of fetal
or maternal instability
• Consider hemodynamic
monitoring during labor
and delivery
• Early delivery for clinical
and hemodynamic
deterioration
HIGH-RISK HEART DISEASE (HRHD) IN PREGNANCY
Elkayam, U. et al. J Am Coll Cardiol. 2016;68(4):396–410.
Management strategies for women who have valve disease, complex congenital heart disease, pulmonary hypertension, aortopathy, and dilated cardiomyopathy.
ASI ¼ aortic size index; BAV ¼ bicuspid aortic valve; echo ¼ echocardiographic; HRHD ¼ high-risk heart disease; MFS ¼ Marfan syndrome; RV ¼ right ventricular.
Elkayam et al. J A C C V O L . 6 8 , N O . 4 , 2 0 1 6
Pregnancy and Heart Disease: Part I J U L Y 2 6 , 2 0 1 6 : 3 9 6 – 4 1 0
398