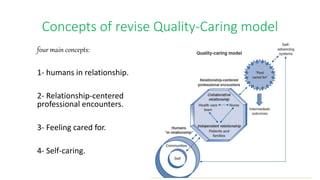
The document provides an overview of Joanne Duffy's Quality Caring Model. It discusses Duffy's background, education, and career achievements. It then outlines the key concepts of the revised Quality Caring Model, including that humans exist in relationships, relationship-centered professional encounters, feeling cared for, and self-caring. The assumptions and propositions of the model are presented. The caring factors and relationships are explained, including with self, patients/families, healthcare team, and communities. The application and critique of the Quality Caring Model are also summarized.