Downloaded 99 times
![Tobacco
Use
• Tobacco
was
responsible
for
more
than
100
million
deaths
worldwide
in
the
20th
century
and
is
forecast
to
kill
at
least
one
billion
more
in
the
century
to
come
[1]
– 80%
of
such
deaths
are
projected
to
occur
in
the
developing
world
[2]
• Half
of
the
current
smokers
today
(about
650
million
people)
will
die
as
a
result
of
tobacco
use,
with
tobacco
use
accounNng
for
the
premature
death
of
4.9
million
people
worldwide
[3].
1. World
Health
OrganizaNon:
WHO
Report
on
the
global
tobacco
epidemic,
2008:
The
MPOWER
Package.
Geneva,
CH:
World
Health
OrganizaNon;
2008.
2. Sabrie
E,
Glantz
SA:
The
tobacco
industry
in
developing
countries.
BriJsh
Medical
Journal
2006,
332:313-‐314.
3. Shafey
O,
Dolwick
S,
Guindon
GE
(Eds.):
Tobacco
Control
Country
Profiles
2003.
Atlanta,
GA:
American
Cancer
Society;
2003.](https://image.slidesharecdn.com/ehealthbehaviourchange-091112070013-phpapp02/75/E-Health-Behaviour-Change-9-2048.jpg)



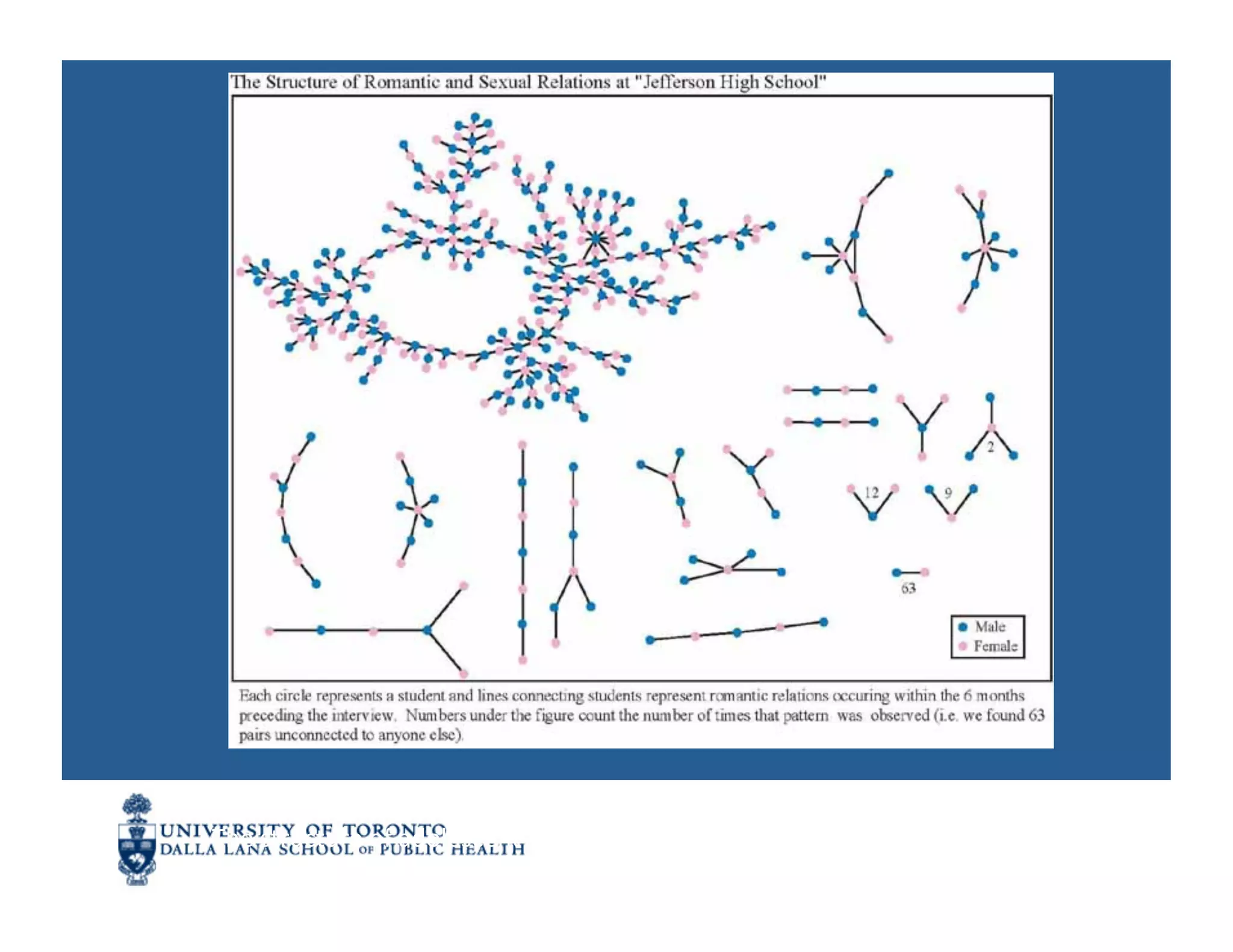
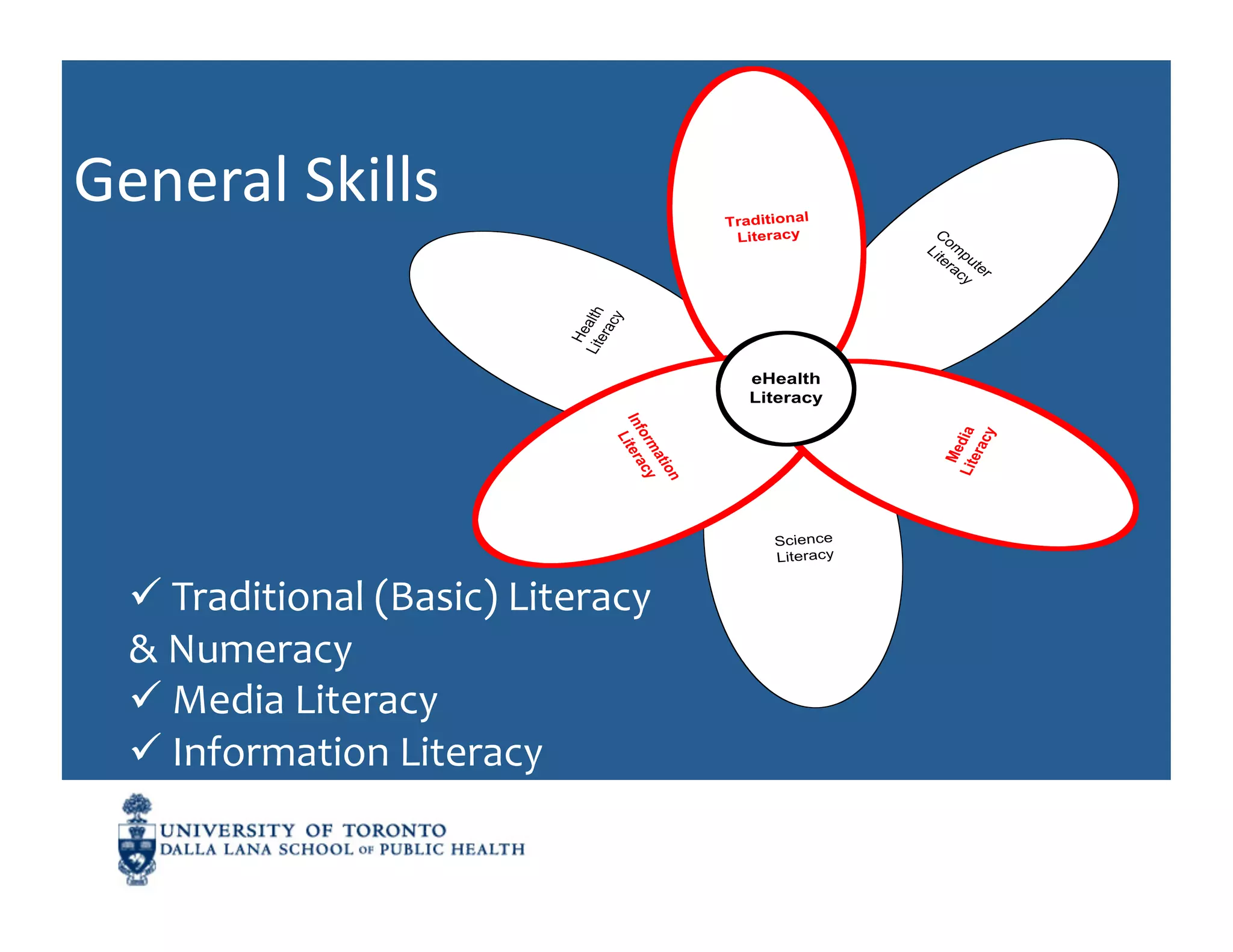
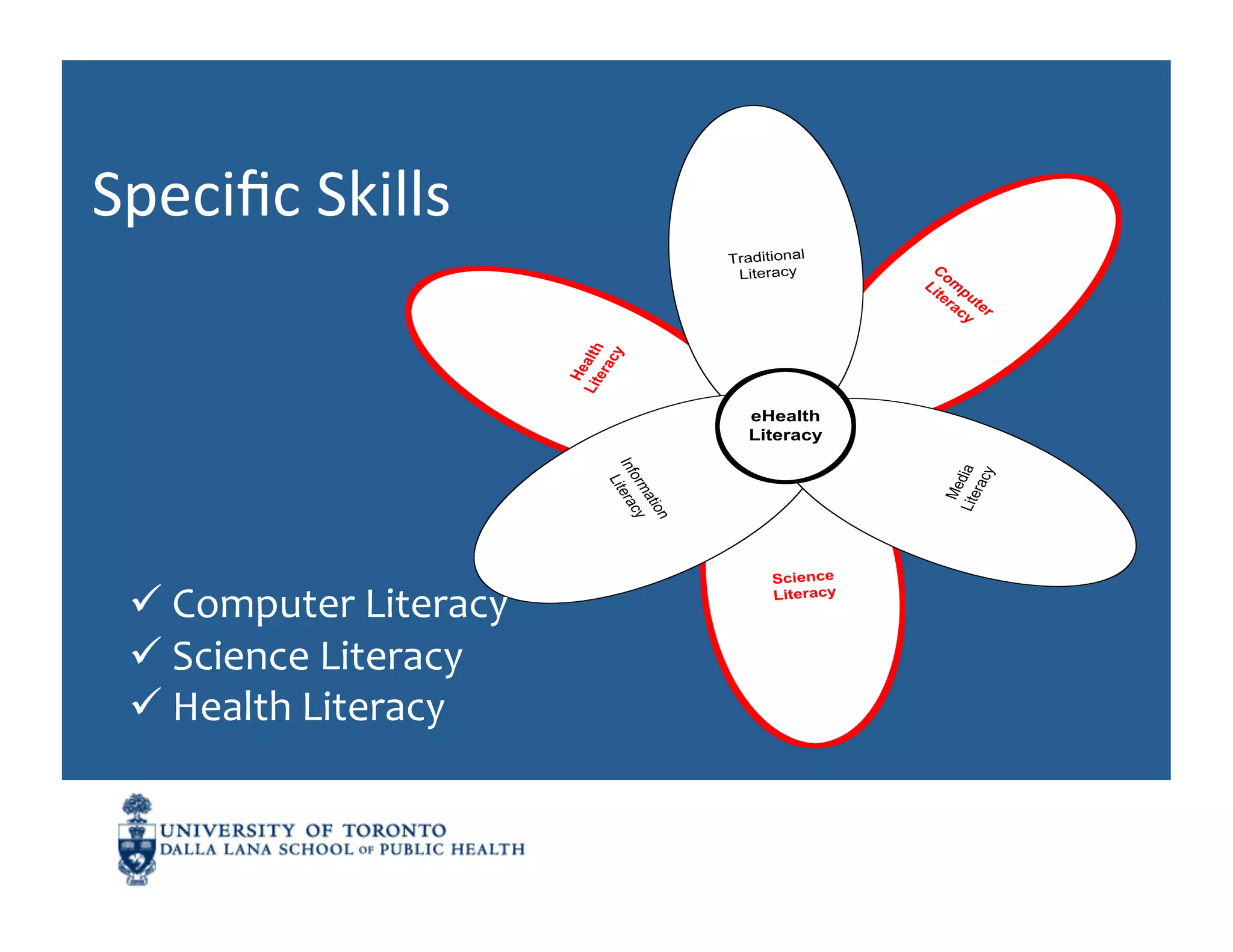
![Literacy
as
a
Tool
for
CommunicaNon
• Literacy
refers
to
a
person’s
ability
to
communicate
at
a
level
that
allows
them
to
understand
the
world
around
them
[interpret
the
signals
coming
in]
and
to
contribute
to
that
world
through
personal
expression
that
is
meaningful
to
others
[sending
useful
signals
out]](https://image.slidesharecdn.com/ehealthbehaviourchange-091112070013-phpapp02/75/E-Health-Behaviour-Change-53-2048.jpg)

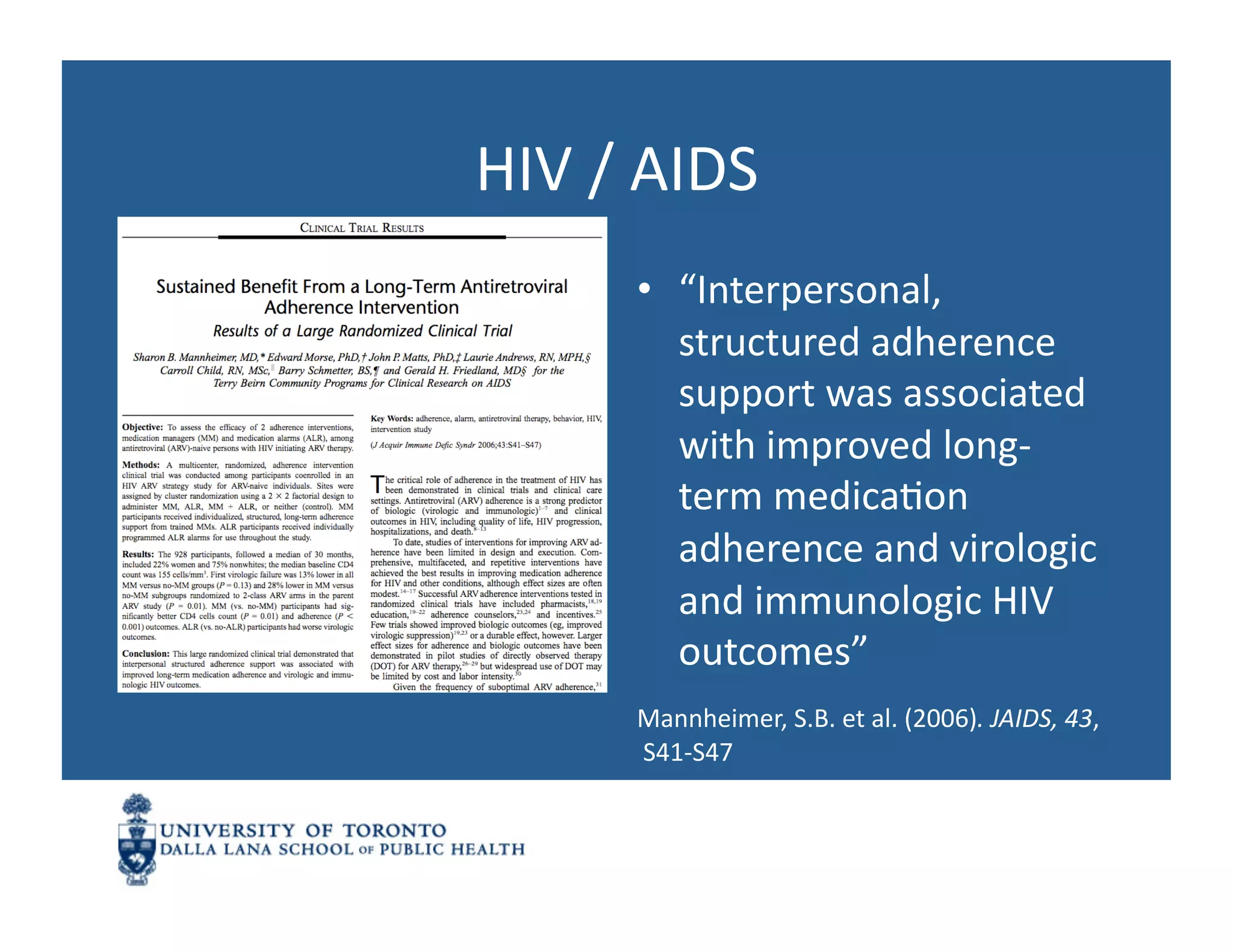
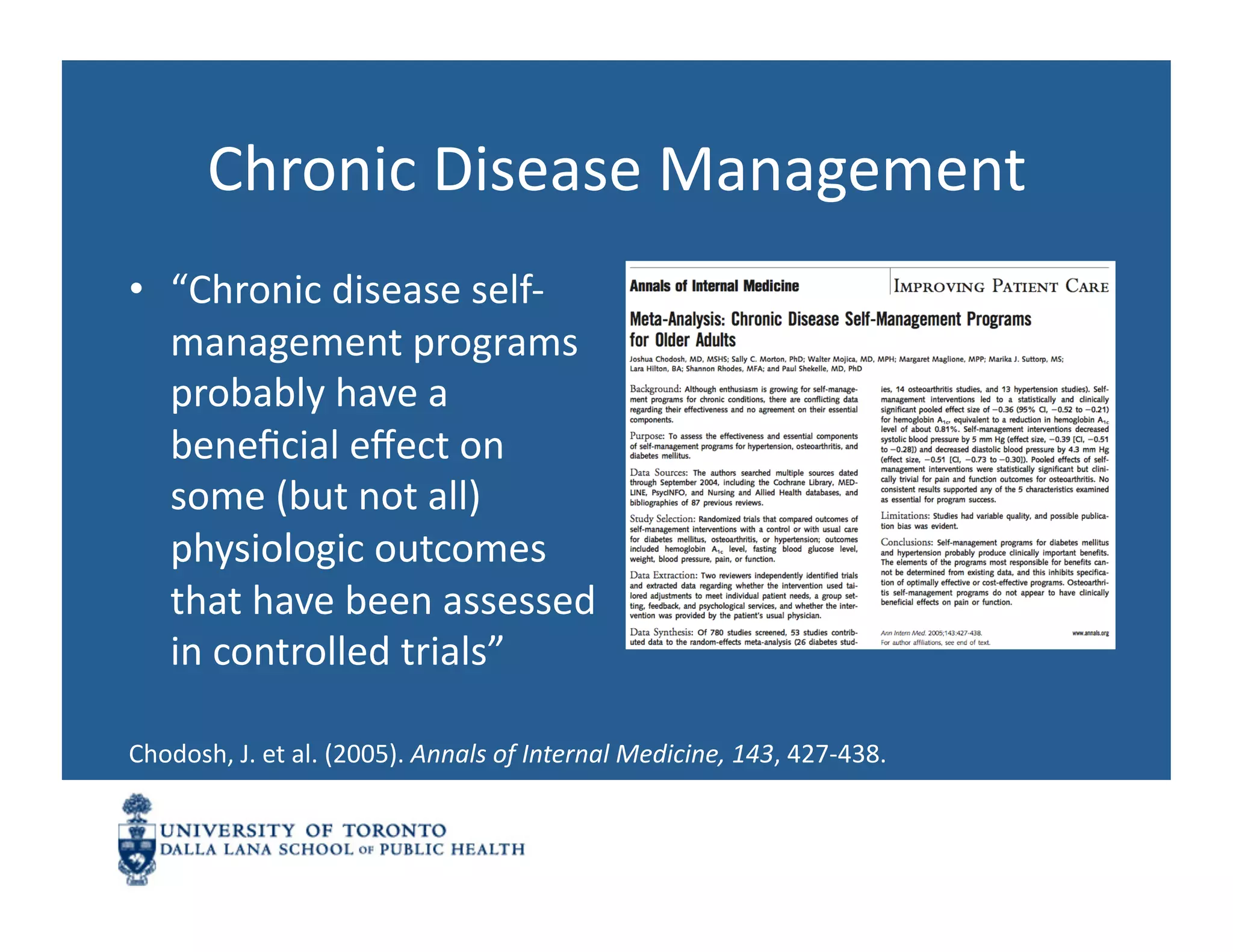
The document discusses the impact of information and communication technologies (ICT) on personal and population health, highlighting significant public health achievements and the importance of behavior change in reducing health risks, such as smoking and obesity. It presents various models and theories of behavioral change, alongside case studies demonstrating the efficacy of web-based interventions in promoting smoking cessation among youth. Additionally, it underscores the need for effective health literacy to enable individuals to seek and understand health information, ultimately improving health outcomes.












![Physical exercise & mental health [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexercisementalhealthautosaved-220301093325-thumbnail.jpg?width=640&height=640&fit=bounds)



![Obesity Final Paper [402119]](https://cdn.slidesharecdn.com/ss_thumbnails/6a3503c0-ed46-49fd-ab98-456b356bdeee-160113180021-thumbnail.jpg?width=640&height=640&fit=bounds)