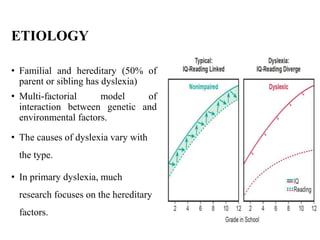
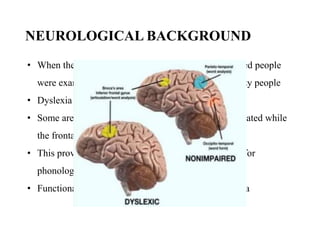
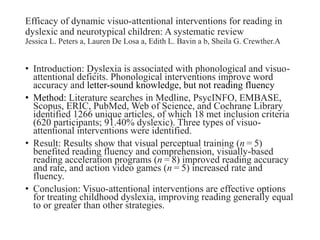
The document discusses dyslexia, a common learning disability characterized by difficulties in reading, spelling, and speaking due to phonological processing issues, and emphasizes the importance of early diagnosis and intervention. It outlines various types of dyslexia, risk factors, and symptoms, detailing both educational techniques and treatment options, including phonics interventions and assistive technology. Additionally, it presents findings on visuo-attentional interventions that can enhance reading fluency and comprehension in dyslexic children.



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



