Downloaded 924 times



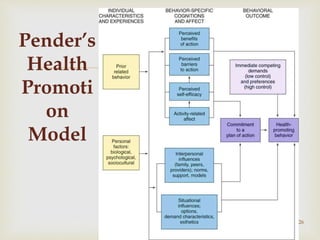



The document discusses Nola Pender's Health Promotion Model (HPM), which emphasizes the multidimensional nature of health and the importance of individual behavior in disease prevention and promotion of a healthy lifestyle. It outlines the model's background, key assumptions, major concepts, and propositions that influence health behaviors, highlighting the role of personal and environmental factors in shaping health-related decisions. Additionally, it provides insights into the model’s applicability in nursing practice and its significance for health promotion across various settings.


































![[Type here]Ok. This school makes me confused. The summary of t.docx](https://cdn.slidesharecdn.com/ss_thumbnails/typehereok-221209051734-656ae2ec-thumbnail.jpg?width=640&height=640&fit=bounds)



















































