Download to read offline




![David S. Robinson, Ed.D. Faculty, Simmons College School of Social Work [email_address] President, DSRobinson & Associates 903 Providence Place, #155 Providence, RI 02903 O: 401-383-7953 M: 617-733-5979 [email_address] www.evaluationhelp.com](https://image.slidesharecdn.com/cdc-presentation-1253444758-phpapp02/85/DSRA-29-320.jpg)

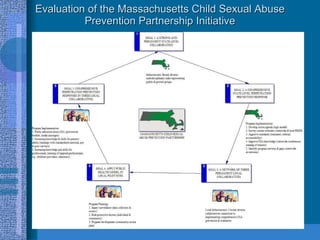
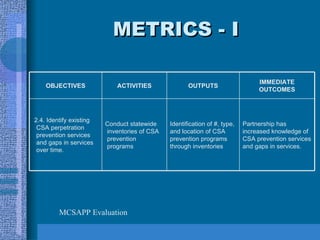
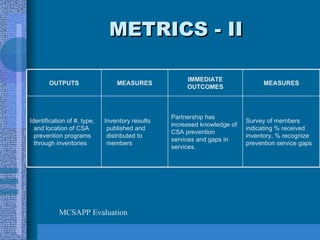
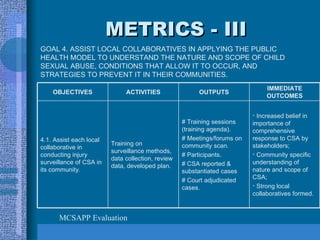
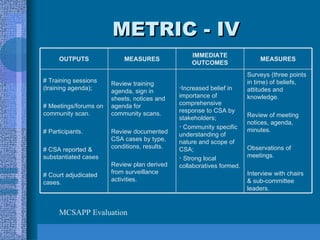
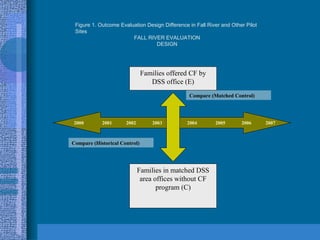
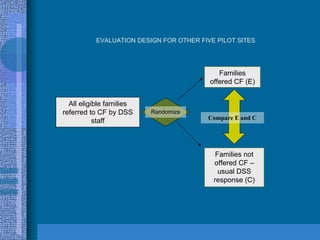
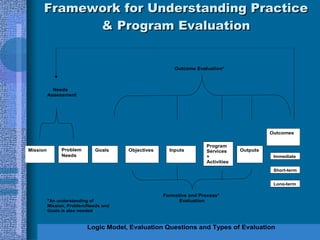
This document discusses evaluation practices and challenges in violence prevention. It provides examples of evaluations conducted on child sexual abuse prevention programs in Massachusetts and shaken baby syndrome prevention programs. It also discusses using evaluation to promote sustainability, dissemination, and teaching evaluation practices to social workers. Key challenges discussed include understanding stakeholder culture and complexity in real-world settings.





















































