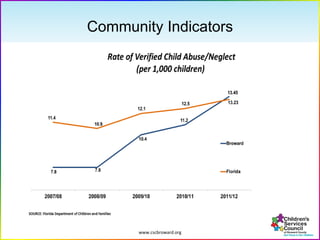
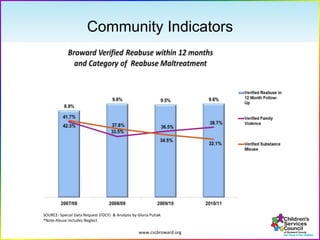
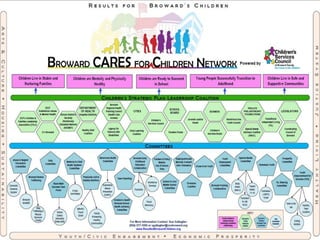
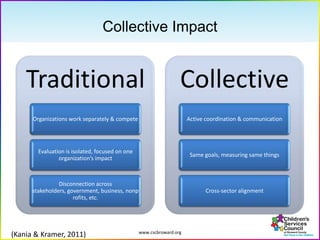
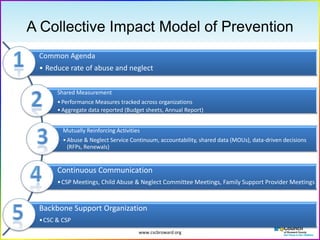
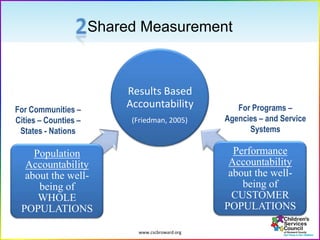
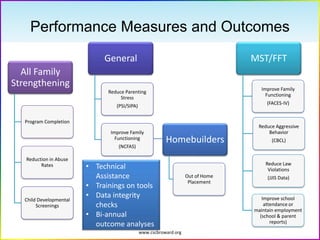
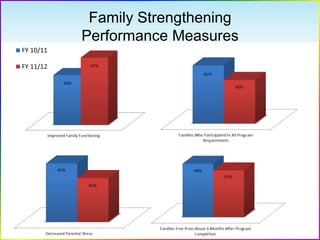
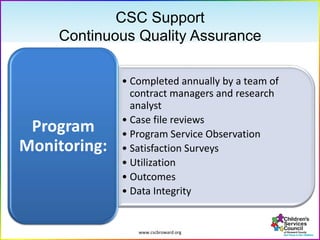
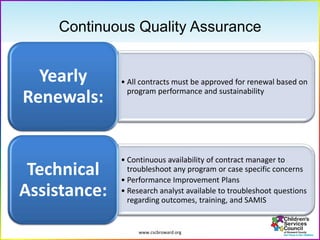
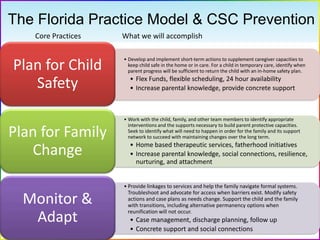
The document outlines a collaborative model for child welfare in Broward County, emphasizing a prevention-focused approach to reduce child abuse and neglect. It highlights the establishment of a shared agenda among various organizations, relying on data-driven decision-making and continuous communication to support families in need. The report also details performance measures and programs aimed at strengthening families and providing necessary resources and support.