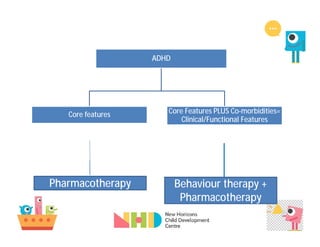
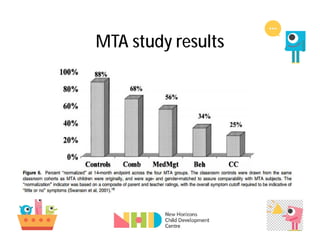
The document discusses ADHD as a syndrome characterized by hyperactivity, impulsivity, and inattention, with a focus on the necessity of a multi-dimensional treatment approach that includes pharmacotherapy and behavioral therapy. It highlights the importance of addressing co-morbidities and the need for a structured, goal-oriented program to ensure effective management. Key studies, including the MTA study, are referenced to analyze the efficacy of combined treatment strategies and the challenges associated with ADHD medication adherence.

![New Horizons Child Development Centre
Data
1301
547
422
128
0
200
400
600
800
1000
1200
1400
2009-2012 2013-2015
Numberofchildren
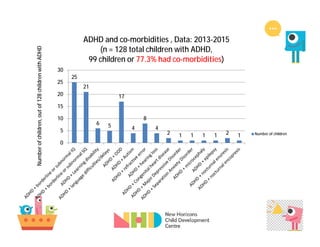
Children with ADHD in 2009-12 (TISS_NHCDC Study) & 2013-2015;
and mean age [2013-15 data analysis is ongoing]
Total children
Children with ADHD
32.4%
23.4%
6.9 years
7.1 years](https://image.slidesharecdn.com/drugsinadhd-160523111538/85/Drugs-in-ADHD-9-320.jpg)



































![ADHD (best)]](https://cdn.slidesharecdn.com/ss_thumbnails/bykhaihojoshuagabriel1-1234763718979961-1-thumbnail.jpg?width=640&height=640&fit=bounds)































