Downloaded 636 times





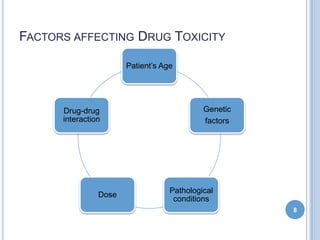

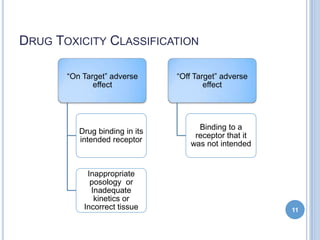






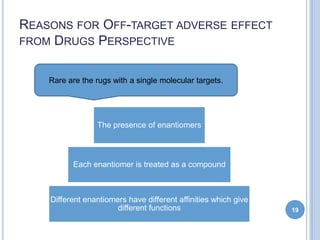











This document discusses drug toxicity and its underlying mechanisms. It covers several topics: - Drug toxicity can occur through both on-target and off-target adverse effects as drugs may bind to unintended receptors. Factors like dosage, genetics, and drug interactions influence toxicity. - On-target effects arise from exaggerated pharmacologic action on the intended receptor. Off-target effects occur when a drug binds unrelated receptors. - Drugs and their metabolites may also cause toxicity. For example, acetaminophen is normally detoxified but high doses overwhelm the pathways, allowing a toxic metabolite to accumulate and damage liver cells. - The document uses examples like statins, antihistamines, and thalidom



































































