Downloaded 74 times

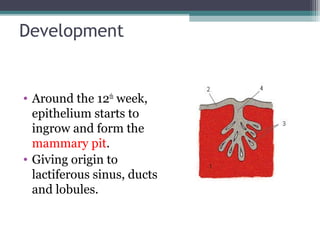
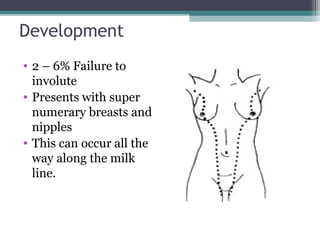
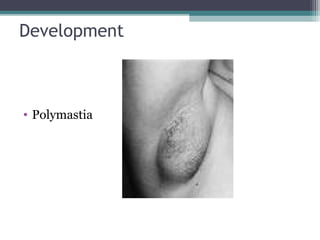
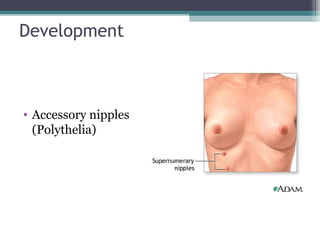
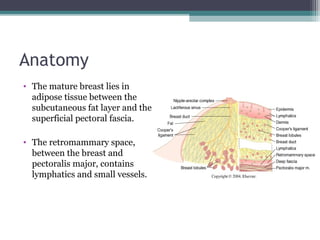
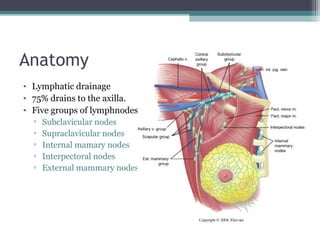
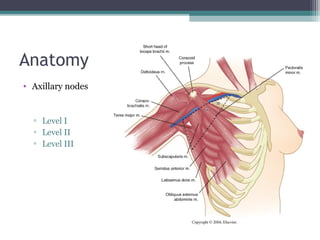
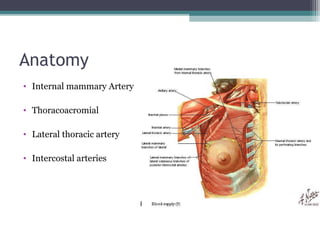

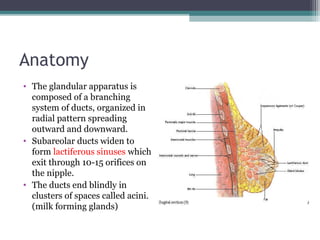
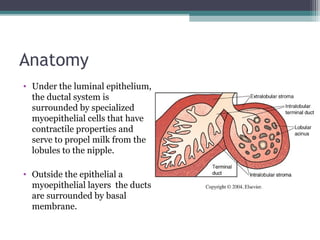
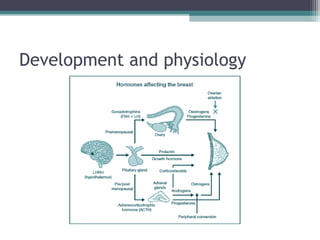




The document discusses the anatomy, physiology, and development of the breast from embryological development through adulthood, as well as several benign clinical conditions that can present in the breast including mastalgia, nipple discharge, breast abscesses, cysts, fibroadenomas, and gynecomastia. It provides details on the histology, presentation, workup, and treatment for each benign condition.









































































