Lung abscess
• Isa localized area of destruction of lung parenchyma
cause by infection of pyogenic organisms results in tissue
necrosis and suppuration.
• It manifests radiological as a cavity with an air-fluid
levels.
• 75% of abscess occur in posterior segment of the Rt. upper
lobe or Apical segments of either lower lobe.
3.
Classification
May beprimary or secondary
Primary : abscess in previously healthy patient or
in a patient at risk for aspiration
Secondary : associated bronchogenic neoplasm or
immunocompromised patient
4.
Risk factors /causes
Infectious agent generally cause lung abscess:
1) Gram negative organisms as klebsiella, S. aureus, & anaerobic
bacilli.
2) T.B
3) Parasitic
4) Fungal disease of the lung as Histoplasma capsulatum, Aspergillus,
Candida
Actinomyces israeli –single large lung abscess:
Lung infiltrate with honey comb of small abscess cavities that may
communicate with chest wall with bony destruction and sinus
formation
HIV infection
5.
Risk factors /causes
1) Most lung abscess are caused by aspiration of material from the GI tract in to
the lungs
Risk factors for aspiration include:
Alcoholism
Seizure
Strock-Depressed conscious level
Neuromuscular disorders
Drug overdose, Sedation
General anasthesia, Impaired laryngeal closure ( cuffed endotracheal tube),
tracheostomy tube, recurrent laryngeal nerve palsy )
Disturbances of swallowing, Delayed gastric emptying
Risk factors /causes
3) Poor oral health: gum disease are more likely to get an
abscess, Dental / periodontal sepsis
4) Paranasal sinus infection
5) Poor immune system : like fungi or the bacteria that
cause T.B , Strep throat, & MRSA.
8.
Risk factors /causes
6) Blood-borne causes: It’s rare, but bacteria or infected blood clot can travel
through bloodstream to the lung, where they cause an abscess.
Hematogenous spread from a distal site:
1. UTI
2. Abdominal sepsis
3. Pelvic sepsis
4. Infective endocarditis
5. IV drug abuse
6. Infective IV canulae
7. Septic thrombophlebitis
9.
Clinical manifestation
Symptomsof a lung abscess commonly come slowly over weeks
to months. They may include:
Cough with purulent sputum
(Sputum is a mixture of saliva & mucous with pus that’s often sour-tasting, foul
smelling, or streaked with blood)
Haemoptysis
Fever, Chills & night sweats
Fatigue & loss of appetite
Pleuritic chest pain
Dyspnoea
Weight loss
10.
Clinical manifestation
Onexamination: No signs specific for lung abscess
Digital clubbing – develop within a few weeks if treatment is
inadequate
Dullness on percussion
Decrease breath sound on auscultation over the segment of lung
involved
Crackles
11.
Diagnosis
History andphysical examination
Sputum, pleural fluid and blood culture
AFB sputum smears 3
Bronchoscopy to get samples of sputum or lung tissue
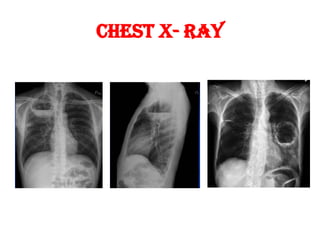
Chest X-Ray
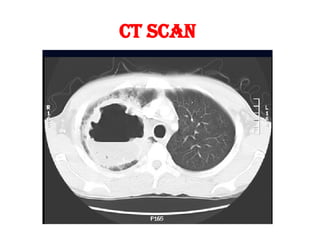
CT Scan
Complications
Chronic abscess:if it longer more than 6 weeks.
Empyema: This is when an abscess breaks into the space
between lungs and chest wall and fills the space with pus.
Bronchopleural fistula
Pneumothorax , pyoneumothorax
sepsis
Metastatic cerebral abscess
Fibrosis, bronchiectasis, amyloidosis
Bleeding: It’s rare, but sometimes an abscess can destroy
a blood vessel and cause serious bleeding.
16.
Management
Medical management:
Rest , good nutrition and adequate fluid intake are supportive
measures to facilitate recovery
Antibiotics
used in large doses, for sufficient time,parentral, broad spectrum for
aerobes and anaerobes ( gm +ve & gm –ve, cocci & bacilli ), and
shift to oral antibiotics after that.
Antibiotics given for prolonged period 4-6 weeks until a chest X-ray
shows the abscess is gone
Penicillin is a drug of choice
Clindamycin has been shown to be superior to penicillin and is the
standard treatment for anaerobic lung infection
17.
Management
Drainage: ifthe abscess is 6 centimeters or more in
diameter.
Chest physiotherapy and postural drainage are helpful in
disease process.
Bronchoscopy, for drainage (tamponade, or removal of
FB ).
Transthoracic needle aspiration ( with toilet and local
antibiotic injection ).
Intercostal tube drainage
18.
Management
Surgery:
It’srare, but some people need surgery to remove the part of the lung
with the abscess.
Surgery is indicated in poor response to antibiotic therapy
Large abscess > 6cm in diameter
Resistance organisms as P. aeruginosa
Massive or recurrent life threatening haemoptysis.
Complicating Empyema.
Suspicion of lung cancer.
Surgery can also help to remove a foreign object
The usual procedures is lobectomy or pneumonectomy