Chest pain
Done by:Nosiba Abd ulraof Alzobiry
Supervisor: Dr/Mokhtar Alnahary
2.
Introduction:-
*Chest pain isamong the most common reasons for which patients
present for medical attention at either an emergency department (ED)
or an outpatient clinic.
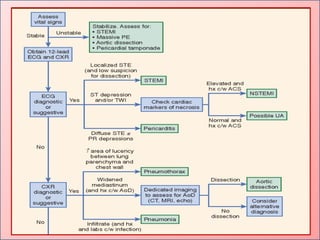
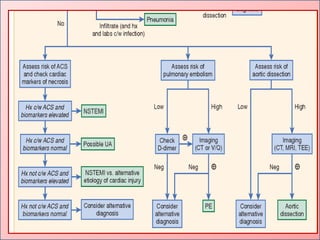
*It is helpful to frame the initial diagnostic assessment and triage of
patients with acute chest discomfort around three catagories:
(1) myocardial ischemia.
(2) other cardiopulmonary causes (myopericardial disease, aortic
emergencies, and pulmonary conditions)
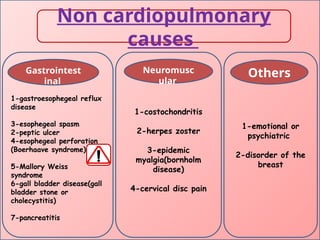
(3) non cardiopulmonary causes.
*Fewer than 15% of evaluated patients are eventually diagnosed with
acute coronary syndrome (ACS) .
*The most common diagnoses are gastrointestinal causes(42%)
3.
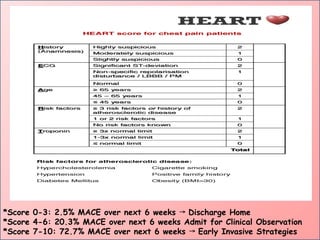
*Score 0-3: 2.5%MACE over next 6 weeks Discharge Home
→
*Score 4-6: 20.3% MACE over next 6 weeks Admit for Clinical Observation
*Score 7-10: 72.7% MACE over next 6 weeks Early Invasive Strategies
→
4.
The EDACS Score(Emergency Department
Assessment of Chest Pain Score)
• is a clinical tool used to assess the risk of acute
coronary syndrome (ACS) in patients presenting with
chest pain. It helps emergency department (ED)
physicians make decisions about which patients can be
safely discharged and which ones need further testing or
admission.
The Vancouver Chest Pain Rule**
• is a clinical decision tool designed to help emergency
department (ED) physicians determine which patients
presenting with chest pain are at low risk for acute
coronary syndrome (ACS) and can be safely discharged
without further cardiac testing. This rule aims to reduce
unnecessary admissions and testing, streamlining care for
patients with chest pain.
5.
What are thesources of the chest pain(anatomic
locations):
.The chest wall including the ribs,the muscles and the
skin.
.The back including the spine,the nerves and the back
muscles.
. The lung,the pleura and the trachea .
.The heart and the pericardium.
.The aorta, the esophagus and the diaphragm.
.Referred pain from the abdominal cavity .
6.
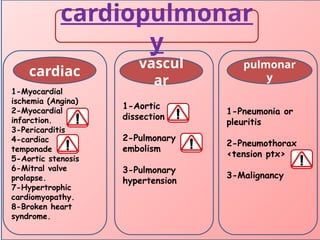
Causes of chestpain
Nontrumatic
cardiopulmonary Non cardiopulmonary
trumatic
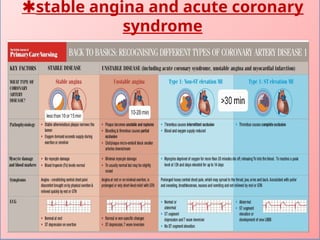
Myocardial infarction:-
Clinical manifestation:-
-Acuteretrosternal chest pain:
Typical: dull, squeezing pressure and/or tightness,
Commonly radiates to left chest, arm, shoulder,
neck, jaw, and/or epigastrium.
-Precipitated by exertion or stress.
Physical examination:-
-Patient is restless,anxious,pallor,
B.p and H.R may be normal or mildly raised
-(Levine’s sign)
-Sign of complication.
11.
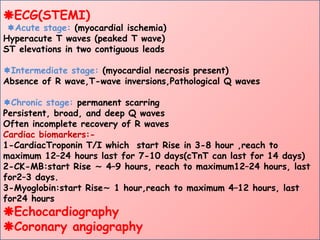
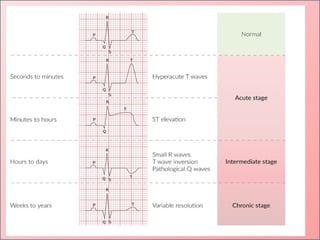
ECG(STEMI)
Acute stage: (myocardialischemia)
Hyperacute T waves (peaked T wave)
ST elevations in two contiguous leads
Intermediate stage: (myocardial necrosis present)
Absence of R wave,T-wave inversions,Pathological Q waves
Chronic stage: permanent scarring
Persistent, broad, and deep Q waves
Often incomplete recovery of R waves
Cardiac biomarkers:-
1-CardiacTroponin T/I which start Rise in 3-8 hour ,reach to
maximum 12–24 hours last for 7-10 days(cTnT can last for 14 days)
2-CK-MB:start Rise 4–9 hours, reach to maximum12–24 hours, last
∼
for2–3 days.
3-Myoglobin:start Rise 1 hour,reach to maximum 4–12 hours, last
∼
for24 hours
Echocardiography
Coronary angiography
13.
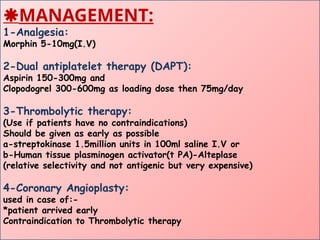
MANAGEMENT:
1-Analgesia:
Morphin 5-10mg(I.V)
2-Dual antiplatelettherapy (DAPT):
Aspirin 150-300mg and
Clopodogrel 300-600mg as loading dose then 75mg/day
3-Thrombolytic therapy:
(Use if patients have no contraindications)
Should be given as early as possible
a-streptokinase 1.5million units in 100ml saline I.V or
b-Human tissue plasminogen activator(t PA)-Alteplase
(relative selectivity and not antigenic but very expensive)
4-Coronary Angioplasty:
used in case of:-
*patient arrived early
Contraindication to Thrombolytic therapy
14.
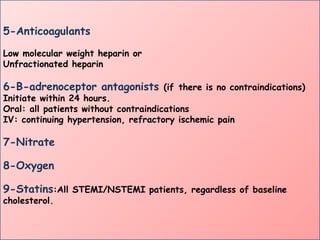
5-Anticoagulants
Low molecular weightheparin or
Unfractionated heparin
6-B-adrenoceptor antagonists (if there is no contraindications)
Initiate within 24 hours.
Oral: all patients without contraindications
IV: continuing hypertension, refractory ischemic pain
7-Nitrate
8-Oxygen
9-Statins:All STEMI/NSTEMI patients, regardless of baseline
cholesterol.
15.
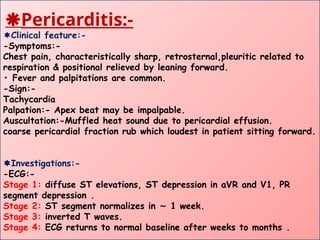
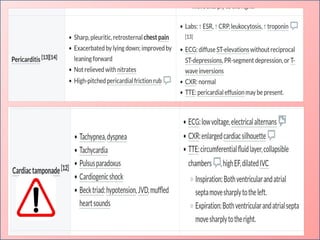
Pericarditis:-
Clinical feature:-
-Symptoms:-
Chest pain,characteristically sharp, retrosternal,pleuritic related to
respiration & positional relieved by leaning forward.
• Fever and palpitations are common.
-Sign:-
Tachycardia
Palpation:- Apex beat may be impalpable.
Auscultation:-Muffled heat sound due to pericardial effusion.
coarse pericardial fraction rub which loudest in patient sitting forward.
Investigations:-
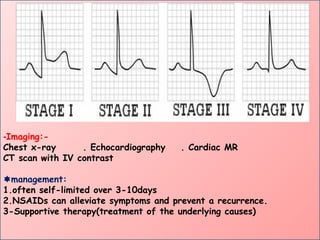
-ECG:-
Stage 1: diffuse ST elevations, ST depression in aVR and V1, PR
segment depression .
Stage 2: ST segment normalizes in 1 week.
∼
Stage 3: inverted T waves.
Stage 4: ECG returns to normal baseline after weeks to months .
16.
-Imaging:-
Chest x-ray .Echocardiography . Cardiac MR
CT scan with IV contrast
management:
1.often self-limited over 3-10days
2.NSAIDs can alleviate symptoms and prevent a recurrence.
3-Supportive therapy(treatment of the underlying causes)
18.
Aortic dissection:
Risk factorsor Etiologies:
-Hypertension
-Trauma, e.g( deceleration injury or iatrogenic injury during valve
replacements or graft surgery)
-Vasculitis with aortic involvement as syphilis .Atherosclerosis
-Congenital as
Connective tissue disease (Marfan syndrome)
Bicuspid aortic valve (e.g., in Turner syndrome)
-Coarctation of the aorta
-Third-trimester pregnancy
Manifestation:
Sudden and severe tearing/ripping pain often radiating to the back
between shoulder blades Syncope, diaphoresis, confusion, or agitation
Hypertension or hypotension
Asymmetrical blood pressure and pulse readings between limbs
19.
Investigation:
-ECG
Normal findings
Signs ofleft ventricular hypertrophy
Nonspecific changes, such as ST depression and T-wave changes
-Laboratory studies
D-dimer: elevated levels
-Chest x-ray
Often normal but may show
Widened mediastinum
Alteration of the mediastinal contour seen on serial imaging
Mediastinal mass
-Transesophageal echocardiography
Investigations of choice are( CT or MR angiography)
Management:
Initial management
pain control and antihypertensive treatment
Stanford A dissection: immediate surgery.
Stanford B dissection: treat conservatively
Supportive care
20.
Pulmonary embolism
Risk factor:-
-InPMH:- H/O Trauma, fracture, surgery.
*H/O prolonged immobility.
*H/O previous DVT
*Drug history (hormonal therapy or OCP).
*H/o malignancy
-Social H/o:-Smoking.
-Family:- FH +ve.
Clinical features:-
-Sudden onset dyspnea is the most common symptom
-Pleuritic chest pain(Acute, sharp retrosternal pain caused by
inflammation of the parietal pleura Typically aggravated by coughing,
swallowing, or deep inspiration)
-Cough, Hemoptysis (occurs in 10-15% of pts.).
-Syncope especially in massive pulmonary embolism.
Non specific Signs:-
-Tachypnea: the most common sign.
-Tachycardia.
-Low grade fever
Chest exam usually normal
21.
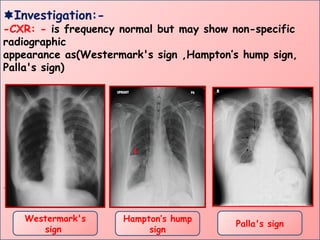
Investigation:-
-CXR: - isfrequency normal but may show non-specific
radiographic
appearance as(Westermark's sign ,Hampton’s hump sign,
Palla's sign)
.
Westermark's
sign
Palla's sign
Hampton’s hump
sign
22.
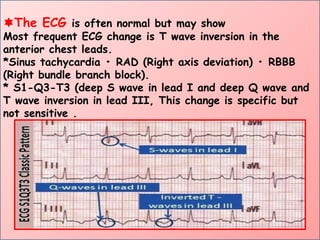
The ECG isoften normal but may show
Most frequent ECG change is T wave inversion in the
anterior chest leads.
*Sinus tachycardia • RAD (Right axis deviation) • RBBB
(Right bundle branch block).
* S1-Q3-T3 (deep S wave in lead I and deep Q wave and
T wave inversion in lead III, This change is specific but
not sensitive .
23.
*Cardiac enzyme:
The serumtroponin I may be elevated, reflecting right
heart strain
*Arterial blood gas (ABG):
Often normal
Common findings
Hypoxemia (e.g., SaO2, PaO2 < 80 mm Hg)
↓
Respiratory alkalosis
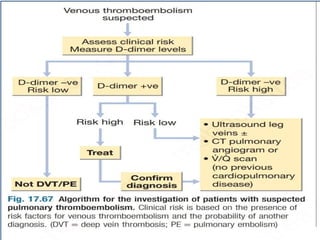
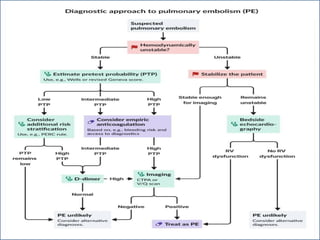
*D-dimer: if normal the PE is very unlikely or exclude in
low risk pt. only. If positive not
confirm(GOOD NEGATIVE)
*VQ scan
*CTPA(CT of the pulmonary arteries with intravenous
contrast) is the first-line diagnostic test
*Pulmonary-angiography (Gold standard) But done only if
other test are equivocal (invasive)
25.
Management:
-Stabilize the pt.ABC.
-Analgesia .
-Anticoagulation: In pts. With suspected DVT or PE
anticoagulant therapy
(should be started immediately)
-Thrombolytic are used only in Pts. with massive PE if
contraindicated then inferior vena cava filter used.
27.
Pneumothorax
Clinical features:-
-Sudden, severe,and/or stabbing, pleuritic chest pain +
Dyspnea is the most-common presentation.
General examination:-
-(tachypnea, May cyanosis, pulses Paradoxus,decrease
blood pressure).
Chest examination:-
-*Inspection: RR , decreased chest expansion in affected
sid.
*Palpation: decreased chest expansion in affected side +/-
Mediastinal deviation,decreased ofTVF.
*Percussion: Hyper-resonant on affected side.
*Auscultation:Absent breath sounds on affected side, no
added sound.
28.
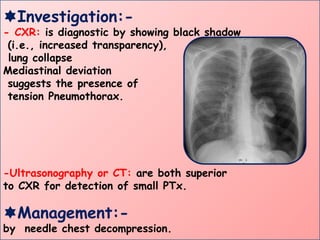
Investigation:-
- CXR: isdiagnostic by showing black shadow
(i.e., increased transparency),
lung collapse
Mediastinal deviation
suggests the presence of
tension Pneumothorax.
-Ultrasonography or CT: are both superior
to CXR for detection of small PTx.
Management:-
by needle chest decompression.
29.
Pneumonia
Clinical feature:
Main complaintis fever , cough and pleuritic chest pain
Sign:
Increased RR ± tachycardia, hypotension.
Chest examination:-
Inspection :decreased in chest expansion of affected side.
Palpation: decreased in chest expansion of affected side &
No deviation.
TVF is increased.
Percussion: Dullness.
Auscultation: decreased air entry , Crepitation’s +/-
Rhonchi , +ve Egophony.
30.
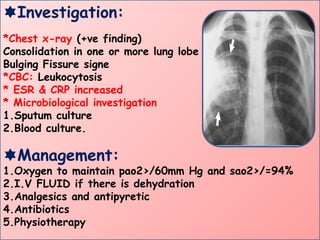
Investigation:
*Chest x-ray (+vefinding)
Consolidation in one or more lung lobe
Bulging Fissure signe
*CBC: Leukocytosis
* ESR & CRP increased
* Microbiological investigation
1.Sputum culture
2.Blood culture.
Management:
1.Oxygen to maintain pao2>/60mm Hg and sao2>/=94%
2.I.V FLUID if there is dehydration
3.Analgesics and antipyretic
4.Antibiotics
5.Physiotherapy
31.
Esophageal perforation:-
Clinical feature:-
-Macklertriad (esp. in Boerhaave syndrome)
1-Vomiting and/or retching.
2-Severe retrosternal pain that often radiates to the back .
3-Subcutaneous or mediastinal emphysema:
crepitus in the suprasternal notch and neck region or crackling sound on
chest auscultation (Hamman sign).
-Dyspnea, tachypnea, tachycardia.
-Dysphagia.
-History of recent endoscopy.
Investigation:-
-Chest x-ray:
Widened mediastinum.
Pneumomediastinum, pneumothorax, pneumoperitoneum,
subcutaneous emphysema .
-Neck x-ray: subcutaneous emphysema.
32.
Management :-
*Initial management:
1-ABCDEsurvey.
2-Nothing by mouth (NPO).
3-IV proton pump inhibitor.
4-Broad-spectrum IV antibiotics.
5-Parenteral analgesia.
*Nonsurgical treatment:
Indications:
Small, contained perforation, demonstrated by:
Either a contained leak with the neck, within the mediastinum, or
between the mediastinum and visceral lung pleura.
*Surgical treatment:
Indications:
Hemodynamic instability.
Patients who do not fulfill the criteria for conservative management .
Clinical deterioration during conservative management.
-Procedure:
Closure of the ruptured esophageal segment.
33.
Esophageal spasm:-
Clinical feature:-
-Chestpain in esophageal spasm:
Non exertional,retrosternal, pressure, tightness or burning pain.may
radiate to back,neck or arm(closely memic angina),prolonged last
between minuet to hours,aggravated by eating quickly, hot or cold
drinking, anxiety or depression, accompanied by heart burn or
dysphagia, relieved by antacid.
Investigation:-
-Upper endoscopy: typically normal in hypermotility disorders
-Esophageal barium swallow:
Distal esophageal spasm: multiple nonperistaltic contractions, which
resemble pseudodiverticula (corkscrew appearance; rosary bead
esophagus
-Manometry.
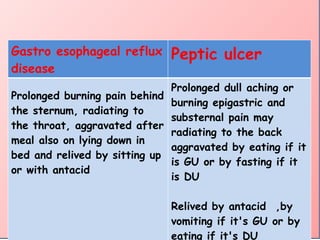
Gastro esophageal reflux
disease
Pepticulcer
Prolonged burning pain behind
the sternum, radiating to
the throat, aggravated after
meal also on lying down in
bed and relived by sitting up
or with antacid
Prolonged dull aching or
burning epigastric and
substernal pain may
radiating to the back
aggravated by eating if it
is GU or by fasting if it
is DU
Relived by antacid ,by
vomiting if it's GU or by
eating if it's DU
36.
Costochondritis
Clinical features:
Sharp, well-localizedpain that is reproducible on palpation of costal
cartilage
History of recent exercise/exertion/chest wall trauma
Diagnostics:
Clinical diagnosis
CXR: normal
Treatment:
-Pain management
-paracetamol
-NSAIDs (e.g., naproxen, ibuprofen)
-Physical therapy (i.e., stretching exercises)
-Reduction of activities that provoke symptoms
-Cough suppressants
37.
Herpes zoster
Clinical features
Severeburning or throbbing pain
Thoracic dermatomes are most commonly affected
Maculopapular rash that develops into a vesicular
rash in a dermatomal distribution
Diagnostics
-Clinical diagnosis
-PCR of vesicle fluid positive for varicella-zoster
virus DNA
Treatment:
Antiviral
38.
Emotional or psychiatricchest pain
Clinical features
- -usually feel like a Retrosternal sharp, stabbing
sensation that starts suddenly, even if a person is
inactive.not radiated pain.more common in women
-No associated esophageal symptoms (e.g., no
heartburn, dysphagia)
(*Diagnosis of exclusion)
Treatment
Reassure the patient.
Referral to psychologist