This study explored the association between digoxin use and mortality in patients with atrial fibrillation (AF), finding that baseline digoxin use did not increase all-cause mortality, but higher serum digoxin concentrations were linked to increased mortality risks, particularly above 1.2 ng/ml. Additionally, initiating digoxin treatment in AF patients was associated with higher mortality and increased rates of hospitalization due to heart failure. The findings suggest that digoxin should be used cautiously and its concentrations monitored closely in AF patients.

![Serum digoxin concentrations and
outcomes
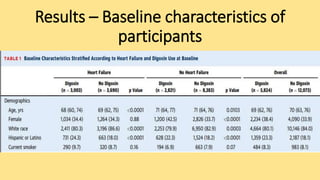
• Serum digoxin concentrations at baseline were measured in 4,434
(76.1%) patients taking digoxin. Baseline characteristics of the
patients with and without digoxin concentration data available were
similar.
• Median serum digoxin concentrations were significantly higher in
patients who died compared with those who survived (median: 0.62
[25th, 75th percentiles: 0.39, 1.01] ng/ml vs. 0.55 [25th, 75th
percentiles: 0.16, 0.86] ng/ml; p < 0.0001).](https://image.slidesharecdn.com/digoxinjournal-191224070612/85/Digoxin-journal-club-21-320.jpg)