



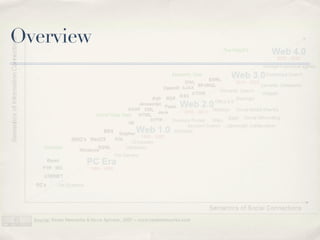
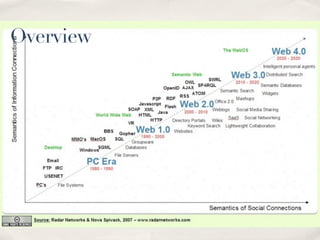















The document discusses the evolution of the internet from Web 1.0 to Web 2.0, highlighting its impact on medical practice and the importance of digital professionalism. It addresses both the opportunities and challenges presented by digital platforms in medical settings, including issues related to confidentiality, ethical behavior, and online persona management. Furthermore, it outlines guidelines for healthcare professionals on navigating social media responsibly to maintain professionalism and protect patient privacy.







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



