Download to read offline
![Overview
MAXIMIZE TABLE TABLE QUIZ
Type 1 vs
Features
Genetics
Positive HLA-DR4 and HLA-DR3 association
Weak familial predisposition
Polygenic
Negative HLA association
Strong familial predisposition
Polygenic
Pathogenesis
Autoimmune destruction of β cells →
absolute insulin deficiency
, progressive destruction
of pancreatic β-cells
Association with obesity No Yes
Onset
Childhood onset typically < 20 years but can
occur at any age
Peaks at age 4–6 years and 10–14 years
Gradual; usually at age > 40 years
C-peptide (insulin) Decreased or absent
Initially elevated, decreased in advanced
stage
Severe Mild to moderate
Insulin sensitivity High Low
Risk of ketoacidosis High Low
β-cells in the islets Decreased Variable (with amyloid deposits)
Classic symptoms (i.e., polyuria, polydipsia,
polyphagia, weight loss)
Common Sometimes
Histology Leukocyte infiltration of islets
Amyloid polypeptide (IAPP) deposits in
islets
Treatment Insulin therapy
Lifestyle changes
Oral antidiabetic drugs
Insulin therapy
COLLAPSE NOTES FEEDBACK
Type 2 diabetes mellitus
Type 1 DM Type 2 DM [1]
[2] [3]
Insulin resistance
Glucose intolerance](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-2-2048.jpg)
![Epidemiology
Prevalence
∼ 1.6 million in the US
∼ 5–10% of all patients with diabetes
Age
Childhood onset typically < 20 years but can occur at any age
Peaks at age 4–6 years and 10–14 years
Race: highest prevalence in non-Hispanic White individuals
Prevalence
∼ 10.5% of adult population in the US
Near 34 million individuals in the US have diabetes with 7.3 million being undiagnosed.
Incidence: ∼ 6.7 per 1,000 among the US adults
Age
Adult onset typically > 40 years
Mean age of onset is decreasing
Gender:
♂
>
♀
Race: highest prevalence in Native Americans, Hispanics, African Americans, and Asian non-Hispanic Americans
Epidemiological data refers to the US, unless otherwise specified.
COLLAPSE NOTES FEEDBACK
Type 1 DM
[4]
[4]
[5]
Type 2 DM
[4]
[4]
[5]
[4]
[4]
The global prevalence of type 2 diabetes has risen substantially in recent years and is expected to continue rising.
The primary reason for this is the rising prevalence of obesity and physical inactivity in industrialized nations.
Insulin production decreases with age.
Prevalence of diabetes mellitus is 13.3% in males and 10.8% in females.](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-3-2048.jpg)
![Etiology
Autoimmune destruction of pancreatic β cells in genetically susceptible individuals
HLA association: HLA-DR3 and HLA-DR4 positive patients are at increased risk of developing .
Associated with other autoimmune conditions
Hashimoto thyroiditis
Type A gastritis
Celiac disease
Primary adrenal insufficiency
Risk factors for type 2 diabetes mellitus
Family history: first-degree relative with diabetes
High-risk race or ethnicity
Dyslipidemia
Prediabetes
Physical inactivity
Cardiovascular disease
Polycystic ovary syndrome
Hypertension
History of gestational diabetes
Other conditions associated with metabolic syndrome and : e.g., severe obesity, acanthosis nigricans
Medications known to increase the risk of diabetes, e.g.:
Glucocorticoids
Statins
Thiazide diuretics
Some HIV medications
Second generation antipsychotics
Type 1 DM [6][7]
T1DM
“If you buy 4 DiaMonds and only pay for 3, you get 1 for free:” DR4 and DR3 are associated with
Diabetes Mellitus type 1.
Type 2 DM [8][9][10]
[10]
[11][12][13]
insulin resistance
Genetic HLA testing can be used to
evaluate the individual risk of inheritance.
Environmental factors (e.g., exposure to
viruses or toxic chemicals) may contribute
to the onset of disease.
Autoimmune gastritis: A form of atrophic gastritis characterized by autoimmune destruction of parietal cells, leading to gland loss, loss of intrinsic factor, achlorhydria, and
vitamin B12 deficiency (pernicious anemia). Associated with other autoimmune diseases (e.g., Hashimoto thyroiditis) and increased risk of gastric adenocarcinoma and type
1 gastric neuroendocrine tumor.
Genetic variants have been identified that increase susceptibility to T2DM. A child with one diabetic parent has a
∼ 40% lifetime risk of developing T2DM. The concordance between monozygotic twins is significant, with some
studies finding rates of > 75%. Environmental factors may render a genetically susceptible person more
vulnerable to the disease; for example, a high-calorie diet and physical inactivity can cause the disease to
manifest earlier.
The following groups are at
increased risk of T2DM: African
Americans, Latinos, Native Americans, Asian Americans, and Pacific Islanders.
HDL level < 35
mg/dL and/or
triglyceride level
> 250 mg/dL
BP ≥ 130/80 mm Hg or patients already on antihypertensive medication
E.g., older nucleoside reverse transcriptase inhibitors and older protease inhibitors
p
2
3
A
13
C
D
I &
·
2
3
1 -
FX .
4 2.
Race
3 .
DisliP
.
3 + obesity
4- obe- + b Phy .
Acti
5- PLoS
6 6.
GDM
7- Pre.
DM
7 PCOS 8 -
CUS Disease .
a-
Drugs
8
9
A
B
C
D](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-4-2048.jpg)
![Classification
Classification according to the WHO and American Diabetes Association (ADA)
Type 1: formerly known as insulin-dependent ( ) or juvenile-onset diabetes mellitus
Autoimmune (type 1A)
LADA: Latent autoimmune diabetes in adults, a variant of diabetes characterized by a late onset of type 1 (autoimmune)
diabetes that is oDen mistaken for .
Idiopathic (type 1B)
Type 2: formerly known as non-insulin-dependent ( ) or adult-onset diabetes mellitus
Gestational diabetes
Other types of diabetes mellitus
MODY ( ): genetic defects leading to β-cell dysfunction
Different forms of autosomal dominant inherited diabetes mellitus that manifest before the age of 25 years and are not
associated with obesity or autoantibodies
Multiple monogenic subtypes (most common: II due to glucokinase gene defect, and III, due to hepatocyte
nuclear factor-1-α gene defect)
II
A single mutation leads to impaired insulin secretion due to altered glucokinase function.
Glucokinase is the glucose sensor of the β cell, facilitating storage of glucose in the liver, especially at high
concentrations.
There is no increased risk of microvascular disease.
Despite stable and chronically elevated HbA levels, II can be managed with diet alone.
All other subtypes, including III, require medical treatment either with insulin or sulfonylureas.
Pancreatogenic diabetes mellitus: following pancreatectomy and due to conditions that lead to destruction of pancreatic
endocrine islets (e.g., hemochromatosis, cystic fibrosis)
Endocrinopathies: Cushing disease, acromegaly
Drug-induced diabetes, e.g., due to corticosteroids (steroid diabetes)
Genetic defects affecting insulin synthesis
Infections (e.g., congenital rubella infection)
Rare immunological diseases: stiff person syndrome
Other genetic syndromes that are associated with diabetes mellitus (e.g., Down syndrome)
COLLAPSE NOTES FEEDBACK
[10][14]
IDDM
type 2 diabetes
NIDDM
maturity-onset diabetes of the young
MODY MODY
MODY
hyperglycemia 1C MODY
MODY
Antibodies have been identified, confirming an autoimmune origin.
Approx. 5–15% of all patients with type 2 diabetes actually have LADA.
The pathogenesis is unclear; autoantibodies are absent. Type 1B appears to have a strong hereditary component.
6
I
A
B
C
2
3
Y
RL ich
ii wh
Is
RL 12
Ty
6](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-5-2048.jpg)
![Pathophysiology
Normal insulin physiology
Secretion: Insulin is synthesized in the β cells of the islets of Langerhans. The cleavage of proinsulin (precursor molecule of insulin) produces
C-peptide (connecting peptide) and insulin, which consists of two peptide chains (A and B chains).
Action: Insulin is an anabolic hormone with a variety of metabolic effects on the body, primarily contributing to the generation of energy reserves
(cellular uptake and metabolism of nutrients) and glycemic control.
Carbohydrate metabolism: insulin is the only hormone in the body that directly lowers the blood glucose level.
Protein metabolism: insulin inhibits proteolysis, stimulates protein synthesis, and stimulates cellular uptake of amino acids
Lipid metabolism: maintains a fat depot and has an antiketogenic effect
Electrolyte regulation: stimulates intracellular potassium accumulation
Type 1 diabetes
Genetic susceptibility and environmental triggers (oGen associated with previous viral infection) → autoimmune response with production of
autoantibodies, e.g., (anti-GAD), (anti-ICA) → progressive destruction
of β cells in the pancreatic islets → absolute insulin deficiency → decreased glucose uptake in the tissues
Type 2 diabetes
Mechanisms
Peripheral insulin resistance
Numerous genetic and environmental factors
Central obesity → increased plasma levels of free faMy acids → impaired insulin-dependent glucose uptake into hepatocytes, myocytes, and
adipocytes
Increased serine kinase activity in fat and skeletal muscle cells → phosphorylation of insulin receptor substrate (IRS)-1 → decreased affinity of
IRS-1 for PI3K → decreased expression of GLUT4 channels → decreased cellular glucose uptake
Pancreatic β cell dysfunction: accumulation of pro-amylin (islet amyloid polypeptide) in the pancreas → decreased endogenous insulin
production
Progression
Initially, is compensated by increased insulin and amylin secretion.
Over the course of the disease, progresses, while insulin secretion capacity declines.
AGer a period of with isolated postprandial , diabetes manifests with fasting .
[15]
[6]
anti-glutamic acid decarboxylase antibody anti-islet cell cytoplasmic antibody
[5]
[16]
[17]
[18]
[1]
insulin resistance
insulin resistance
impaired glucose tolerance hyperglycemia hyperglycemia
Stimulates glucose uptake into cells
and glycogen production; inhibits
glycogenolysis and gluconeogenesis
Stimulates fatty acid uptake into cells and lipogenesis. It inhibits
lipolysis and the β-oxidation of free fatty acids in the liver
Directly stimulates Na+/K+ ATPase and promotes intracellular alkalosis, reduces phosphate
levels (glucose binds to phosphate in the cell), and stimulates magnesium uptake into cells
The absence of the insulin-dependent inhibition of hepatic glycogenolysis and gluconeogenesis further promotes hyperglycemia.
Peripheral insulin resistance creates a huge demand for glucose
lowering hormones, resulting in increased production of pro-insulin
and pro-amylin. The pancreatic proteolytic enzymes that convert
pro-insulin and pro-amylin into insulin and amylin are not able to
keep up with the high levels of secretion, which leads to the
accumulation of pro-amylin.
The exact mechanism by which pro-amylinaggregates
decrease insulin production is not completely understood.
Postprandial hypoglycemia may occur due to reactively elevated insulin secretion,
stimulating rapid glucose uptake into cells (regulatory hyperinsulinemia).
1. Disease progression in type 2 diabet es
2. Consequences of insulin deficiency
4
3
4
y
-
> k+, my
+ 2
- Alkalosis
-
> Pho,
Nat
-
HALDR
-
&
↑ ·
I
x
*](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-6-2048.jpg)
![Clinical features
MAXIMIZE TABLE TABLE QUIZ
Type 2 DM
Onset
O"en sudden
Diabetic ketoacidosis (DKA) is the first manifestation in
25–50% of cases
Children may present with acute illness and classic symptoms
Typically gradual
The majority of patients are asymptomatic.
Some patients may present with a hyperglycemic crisis.
Elderly patients especially may present in a hyperosmolar hyperglycemic state.
Occasionally, patients with present with DKA , which mostly affects black and
Hispanic individuals.
Symptoms of complications may be the first clinical sign of disease.
Clinical
features
Classic symptoms of hyperglycemia
Polyuria, which can lead to secondary enuresis and nocturia in children
Polydipsia
Polyphagia
Nonspecific symptoms
Unexplained weight loss
Visual disturbances, e.g., blurred vision
Fatigue
Pruritus
Poor wound healing
Increased susceptibility to infections
Calf cramps
A thin appearance is typical for patients with .
Possible cutaneous signs of
Benign acanthosis nigricans
Acrochordons
Clinical features of diabetes mellitus
Type 1 DM [1]
[10]
[19]
T2DM
[20]
[21]
T1DM
insulin resistance [22]
Diabetes mellitus should be suspected in patients with recurrent cellulitis, candidiasis, dermatophyte infections, gangrene, pneumonia
(particularly tuberculosis reactivation), influenza, genitourinary infections (UTIs), osteomyelitis, and/or vascular dementia.
Usually diagnosed when routine examinations reveal
elevated blood glucose levels in the urine or blood
Sometimes referred to as ketosis-prone T2DM
Polyuria The production of an abnormally large amount of urine.
Quantitatively defined as the passage of > 3 liters of urine in 24 hours.
In patients with diabetes, glucosuria leads to polyuria; glucose causes osmotic
movement of water into the renal tubules, resulting in increased urination.
Polydipsia A condition of excessive thirst. Can be caused by organic (e.g.,
dehydration, hypovolemia, hyperglycemia, diabetes insipidus) or non-
organic conditions (e.g., psychogenic polydipsia).
Due to excessive thirst secondary to
polyuria and subsequent dehydration
A symptom of excessive hunger and/or thirst.
Significant blood glucose fluctuations may lead to osmotic swelling of the lens and transitory changes in refraction (myopia).
Due to either poor circulation, dry skin, or yeast infections
Muscle cramps are seen more commonly in patients with T2DM than in the general population.
Furthermore, they are more likely to occur in patients who have already developed neuropathy.
1. Acanthosis nigricans
2. Acrochordons (skin tags)
&
I 2](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-7-2048.jpg)
![Screening
Indications for diabetes screening
The indications listed below are consistent with the 2024 ADA guidelines. The 2021 USPSTF guideline recommends screening in adults aged
35–70 years with overweight or obesity.
All individuals ≥ 35 years of age
Patients < 35 years of age who:
Are overweight or obese AND have ≥ 1 of the following risk factors:
First-degree relative with diabetes
High-risk race or ethnicity
Physical inactivity
Cardiovascular disease
Polycystic ovary syndrome
Hypertension
Dyslipidemia
Other conditions associated with : e.g., severe obesity and acanthosis nigricans
Have prediabetes or a history of gestational diabetes
Have any risk-enhancing comorbidities, including:
HIV infection
Cystic fibrosis
Post organ transplantation
Pancreatitis
Consider screening individuals exposed to medications known to increase the risk of diabetes, e.g., statins.
Individuals who are planning pregnancy with any
See “Gestational diabetes” for testing indications during pregnancy.
COLLAPSE NOTES FEEDBACK
[10]
[10][23][24]
insulin resistance
risk factor for T2DM
If results are normal, repeat testing in asymptomatic patients at least every three years. Patients with prediabetes should be tested
annually. Patients with a history of gestational diabetes should be tested at least every three years. [10]
The previous recommended age range for screening was 40 to 70 years of age.
Overweight in Adults with a body mass index ≥ 25–29.9 kg/m², in children is defined as a BMI at or above the 85th percentile.
obese in Adults with a body mass index ≥ 30 kg/m², in Children ≥ 95th percentile.
These criteria also apply to children who are > 10 years of age or those who have already begun puberty (whichever occurs first).
BMI of ≥ 23 kg/m2 in Asian American individuals or a BMI of ≥ 25 kg/m2 in all other individuals
The following groups are at increased risk of T2DM: African Americans, Latinos, Native Americans, Asian Americans, and Pacific Islanders.
BP ≥ 130/80 mm Hg or patients already on antihypertensive medication
HDL level < 35 mg/dL and/or triglyceride level > 250 mg/dL
Oral glucose tolerance test is preferred. HbA1c is not recommended as a screening method in this subgroup of patients.
Screening is also recommended 3–6 monthsafter an episode of acute pancreatitis.
Consider screening all individuals of childbearing potential even in the absence of risk factors.
gestational diabetes typically performed at 24-28 weeks' gestation.
I
2
A
8 Ex.
2
3
Y
1-w
2-
GDm
5 3- Par
4 -
Cf
B
5-Drugf
6- Pregn
E
D
E
F](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-8-2048.jpg)
![Diagnosis
Diagnostic criteria for diabetes mellitus
Random blood glucose level ≥ 200 mg/dL in patients with (i.e., polydipsia, polyuria, polyphagia, unexplained weight
loss) or hyperglycemic crisis
OR ≥ 2 abnormal test results for in asymptomatic individuals
Hyperglycemia tests
Random blood glucose: blood glucose measured at any time irrespective of recent meals
Fasting plasma glucose ( ): blood glucose measured aAer > 8 hours of fasting
Oral glucose tolerance test ( )
One-step OGTT: measurement of and blood glucose 2 hours aAer the consumption of 75 g of glucose
Two-step OGTT: used in diagnosis of gestational diabetes
Nonfasting patients are given 50 g of glucose and blood glucose is measured aAer 1 hour.
If values at 1 hour are ≥130–140 mg/dL , measure and blood glucose 1, 2, and 3 hours aAer the consumption of
100 g of glucose.
For interpretation of results, see “Diagnosis of gestational diabetes.”
Hemoglobin A1C ( or ): , which reflects the average blood glucose levels of the prior 8–12 weeks
Can be measured at any time
Results may be altered by a variety of conditions or treatments, e.g., sickle cell trait, chronic kidney disease.
Factors resulting in a falsely high
Increased RBC lifespan: e.g., iron and/or vitamin B deficiency, splenectomy, aplastic anemia
Altered hemoglobin: chronic kidney disease
Factors resulting in a falsely low
Decreased RBC lifespan: e.g., due to acute blood loss, hemoglobinopathies such as sickle cell trait/disease, thalassemia, G6PD-deficiency,
cirrhosis, hemolytic anemia, splenomegaly, antiretroviral drugs
Increased erythropoiesis: e.g., due to EPO therapy, reticulocytosis, pregnancy (second and third trimesters), iron supplementation
Altered hemoglobin: high-dose vitamin C and E supplementation
[10]
symptoms of hyperglycemia
hyperglycemia
[10]
FPG
OGTT [25]
fasting plasma glucose
fasting plasma glucose
HbA1c A1C glycated hemoglobin
[10][26][27]
HbA1c
12
HbA1c
Significant discrepancy between and glucose measurements warrants investigation of the underlying cause (e.g., sickle cell
trait).
HbA1c
All tests use venous blood plasma.
When used to diagnose gestational diabetes, a blood glucose reading is also taken 1 hourafter consumption of glucose.
The threshold for an abnormal study varies depending on the laboratory.
Patients are not required to fast and the results are independent of time of day. HbA1ccan be measured during critical illness.
HbA1c cannot be considered a reliable tool
in such cases and other results (plasma
glucose levels, glycated serum protein, or
glycated albumin) should be taken into
account when diagnosing and monitoring
diabetes.
Due to high carbamylated hemoglobin
A water-soluble vitamin and enzymatic cofactor for lysyl and prolyl hydroxlases, both of which
are important enzymes in the synthesis of collagen. Vitamin C deficiency results in scurvy.
⑩
!
Y
&](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-9-2048.jpg)
![MAXIMIZE TABLE TABLE QUIZ
Interpretation of hyperglycemia tests
2-hour glucose value a7er
Diabetes mellitus ≥ 126 mg/dL (≥ 7.0 mmol/L) ≥ 200 mg/dL (≥ 11.1 mmol/L) ≥ 6.5%
Prediabetes 100–125 mg/dL (5.6–6.9 mmol/L) = impaired fasting glucose 140–199 mg/dL (7.8–11.0 mmol/L) = impaired glucose tolerance 5.7–6.4%
Normal < 100 mg/dL (< 5.6 mmol/L) < 140 mg/dL (< 7.8 mmol/L) < 5.7%
Additional recommended evaluation
BMP
Renal function
Electrolytes, including potassium
Spot urinary albumin-to-creatinine ratio: to detect microalbuminuria
Significant discrepancy between and glucose measurements warrants investigation of the underlying cause (e.g., sickle cell
trait).
HbA1c
[10]
FPG one-step OGTT HbA1c
Diagnosis of diabetes
mellitus
[28]
eGFR using CKD-EPI
According to the ADA
This cutoff is consistent with the
recommendations of the ADA. Other
organizations, including the WHO, define IFG
as > 110 mg/dL.
HbA1c at this level does not allow for a
definitive diagnosis; an OGTT or
fastingglucose test is necessary to
differentiate between diabetes mellitus,
impaired glucose tolerance, and normal
(healthy) glucose metabolism.
A laboratory test that includes the serum concentrations of several compounds, including sodium, potassium, chloride, bicarbonate, urea nitrogen, creatinine, and glucose. Sometimes also
contains the serum calcium concentration.
Low GFR is suggestive of chronic kidney disease. The calculation is used to evaluate for diabetic nephropathy and is also necessary for medication adjustments
Especially patients on ACE inhibitors, ARBs, or diuretics, who should be assessed
periodically (at least once a year). Increased potassium can also be seen in CKD.
An early sign of diabetic nephropathy. Over
the course of the disease, the level of
albuminuria correlates with the risk of
cardiovascular and renal complications.
I
2](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-10-2048.jpg)
![Additional optional studies
These tests are not routinely indicated or required to establish a diagnosis.
C-peptide: can help differentiate between types of diabetes
↑ C-peptide levels may indicate and hyperinsulinemia →
↓ C-peptide levels indicate an absolute insulin deficiency →
Urinalysis
Glucosuria may be present if the renal threshold for glucose is reached (nonspecific for diabetes mellitus).
Ketone bodies: positive in acute metabolic decompensation (diabetic ketoacidosis)
Microalbuminuria: early sign of diabetic nephropathy
Islet autoantibody testing: Consider in patients with diagnosed diabetes mellitus if there is clinical suspicion for .
Antiglutamic acid decarboxylase antibodies ( ): An antibody against the enzyme glutamic acid decarboxylase, which is responsible for
the conversion of glutamic acid to GABA
Anti-tyrosine phosphatase-related islet antigen 2 (IA-2)
Anti-zinc transporter 8 antibodies
COLLAPSE NOTES FEEDBACK
Differential diagnoses
Glucagonoma
Somatostatinoma
The differential diagnoses listed here are not exhaustive.
COLLAPSE NOTES FEEDBACK
Management
General principles
Main goal: blood glucose control, tailored to glycemic targets and regularly monitored
Patients with always require insulin therapy.
may be managed with noninsulin antidiabetics and/or insulin therapy.
Acute illness may require temporary changes in treatment (e.g., increased insulin demand due to acute stress reaction).
Comprehensive diabetes care (all patients)
Lifestyle modifications, including:
Weight reduction
[29][30]
insulin resistance T2DM
T1DM
[30]
T1DM [10]
Anti-GAD
[30]
[31]
[31]
T1DM
T2DM
Glucosuria can be an unreliable parameter, as it
may occur despite normoglycemia, e.g., due to
tubulointerstitial nephritis, caused by certain
medications including SGLT2 inhibitors, or
physiologically in pregnancy. Glucosuria may also
be absent despite hyperglycemia if the renal
threshold is increased, e.g., in diabetic kidney
disease.
This can include an initial presentation at a
young age, diabetes ketoacidosis at diagnosis,
and absence of risk factors for T2DM.
Detection of IA-2 autoantibodies is extremely variable depending on the age of onset, ranging from < 40% to 80%.
While screening for T1DM with autoantibodies is not routinely recommended, it can be considered for patients with first-degree relatives
with T1DM or in the setting of research trials
Consider specialist consultation if the differentiation between T2DM and T1DMis unclear.
Recommendations are consistent with the 2024 ADA guidelines.
This includes information on necessary lifestyle modifications, glycemic monitoring, medication use, and identifying and handling complications.
3
-
4
S &
&
· # e](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-11-2048.jpg)
![Weight reduction
Balanced diet and nutrition (including a high-fiber diet)
Regular exercise
Smoking cessation
Routine
Evaluation for and management of common comorbidities as indicated
Vaccinations: e.g., influenza, hepatitis B, pneumococcal vaccines, zoster vaccine, and COVID-19.
ASCVD risk assessment and ASCVD prevention, including
Hypertension management
Management of hypercholesterolemia
Patients aged 40–75 years with diabetes mellitus: Initiate moderate-intensity statin therapy, regardless of lipid levels.
Assess indications for high-intensity statins.
Glycemic targets in diabetes
MAXIMIZE TABLE TABLE QUIZ
Common glycemic targets
< 7%: suitable for most patients
Preprandial capillary glucose 80–130 mg/dL (4.4–7.2 mmol/L)
Peak postprandial capillary glucose < 180 mg/dL (< 10.0 mmol/L)
Glycemic monitoring for DM
Home glucose monitoring
Glucose levels can be used to evaluate treatment and prevent hypoglycemia and , especially in patients using insulin.
Self-monitoring of blood glucose (SMBG): at fixed times or as necessary
Continuous glucose monitoring (CGM): Interstitial glucose levels are measured continuously or intermi`ently using a device.
screening for microvascular complications of diabetes
[32][33]
[34]
[34]
[35]
Physical exercise reduces blood glucose and increases insulin sensitivity.
[38][39]
[38]
HbA1c [38][39]
Glycemic targets should be individualized. A target of < 7% is generally suitable for most nonpregnant adults.
HbA1c [38]
[38][40]
hyperglycemia
[40]
Live influenza vaccination is not
recommended for individuals with diabetes.
Atherosclerotic Cardiovascular Disease
Diabetes-specific risk factors include T2DMfor a duration of ≥ 10 years, T1DM for a duration of ≥ 20 years, albumin-to-
creatinine ratio ≥ 30 mg/g, eGFR < 60 mL/min/1.73 m2, retinopathy, neuropathy, and ankle-brachial index < 0.9.
A statin dosage that is expected to reduce LDL by 30-49%. Examples include 5-10 mg of rosuvastatin or 10-20 mg atorvastatin daily.
A statin dosage that is expected to reduce LDL by ≥ 50%. Examples include 20-40 mg of rosuvastatin or 40-80 mg atorvastatin daily.
The following recommendations are consistent with the 2024 ADA guideline.
Consider a more or less stringent target depending
on clinical judgment and patient preference.
Measured 1–2 hours after starting a meal
Assess for past episodes or risk of hypoglycemia regularly and adjust glycemic goals accordingly. Hypoglycemia is one of the major limitations for adequate glycemic control. [38]
In patients that meet preprandial glucose targets, HbA1c above target may be due to postprandial hyperglycemia that requires prandial insulin dose adjustments.
HbA1c is measured at fixed intervals.
1. At least every 6 months if targets are met
2. At least every 3 months in the following situations:
• If targets are not met
• If treatment has recently been modified
• If the patient is undergoing intensive insulin therapy
Monitoring intervals may vary depending on the current pharmacotherapy or recent
therapeutic adjustments, physical activity levels, whether or not the patient is meeting
glycemic targets, hypoglycemia risk, and symptoms.
These measurements can be read by the patient and/or clinician.
YPAP
An
B
Ne
FPG](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-12-2048.jpg)
![Hypoglycemia
Assess for episodes of hypoglycemia (symptomatic or asymptomatic) at every follow-up visit.
Early morning
Early morning may be caused by:
Dawn phenomenon
A physiological increase of growth hormone levels in the early morning hours stimulates hepatic gluconeogenesis and leads to a subsequent
increase in insulin demand that cannot be met in insulin-dependent patients, resulting in elevated blood glucose levels.
Consider measurement of nocturnal blood glucose levels before initiating insulin therapy.
Long-acting insulin dose may be given later or increased under careful glycemic control.
Somogyi effect (widely taught but unproven hypothesis)
Description: Nocturnal hypoglycemia due to evening insulin injection triggers a counterregulatory secretion of hormones , leading to
elevated blood glucose levels in the morning.
There is no evidence to support the existence of this effect.
COLLAPSE NOTES FEEDBACK
Reassess and adjust treatment at regular intervals, e.g., every 3–6 months.
hyperglycemia
hyperglycemia
[41][42][43]
As there is liBle to no evidence to support the existence of the , it should not be assumed that early morning
is due to nocturnal hypoglycemia. Rather, it is more likely caused by nocturnal with or without
hypoinsulinemia and/or the early morning secretion of counterregulatory hormones (e.g., cortisol).
Somogyi effect
hyperglycemia hyperglycemia
[41][42][43]
Differential diagnosis of
early-morning hyper-
glycemia
Prescribe glucagon for individuals taking insulin or at high-risk for hypoglycemicevents
The dawn phenomenon, sometimes called the dawn effect, is an observed increase in blood sugar levels that takes place in the early-morning, often between 2 a.m. and 8 a.m.
Glucagon, epinephrine, cortisol, growth hormones
DP* GH# ↑ glucones. - Insulin?!!
↳> Hypergl .
Epi
So . Ex Insulin Insation -
> Hyogly · cot ·
-N Glucose
Gluco
GH](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-13-2048.jpg)
![Antihyperglycemic treatment
Insulin replacement therapy
Treatment options
Multiple daily insulin injections (see “Full basal-bolus insulin regimen” for details)
Insulin pump (consider for most patients)
Approach
Start treatment in all patients at diagnosis.
Monotherapy with me?ormin is the first-line initial treatment for most patients.
If there are contraindications for meBormin, choose a different noninsulin antidiabetic, depending on patient factors.
Consider early combination pharmacological therapy in select patients
Noninsulin antidiabetics
MAXIMIZE TABLE TABLE QUIZ
Noninsulin antidiabetics for the treatment of type 2 diabetes mellitus
Drug class Examples Important considerations
Biguanides Me?ormin Drug of choice, unless there are contraindications for meBormin
Dipeptidyl peptidase-4
inhibitor
Sitagliptin
Saxagliptin
Linagliptin
Avoid saxagliptin in patients with heart failure.
SGLT-2 inhibitors Empagliflozin
Recommended for patients with CKD and confirmed eGFR 15-29 mL/min/1.73 m2
Consider in patients with clinical ASCVD or high risk of ASCVD, chronic kidney disease, or
congestive heart failure.
Beneficial for patients who need to lose or maintain their weight
Semaglutide
Oral
Type 1 diabetes mellitus
[31]
Type 2 diabetes mellitus
[31]
[31][45]
MeBormin should be part of every patient's treatment, unless contraindicated, and continued for as long as it is tolerated, as it is
safe, effective, widely available, and has been shown to reduce cardiovascular events and mortality. [31]
[31]
1. Starting dose calculation
• Exogenous insulin requirements will depend on the residual insulin production of the pancreas.
• Total daily dose (TDD) of insulin is usually ∼ 0.4–1.0 units/kg per day, divided into 50% basal and 50% prandial insulin.
• Consider initiating treatment with 0.5 units/kg per day.
2. Dose titration
• After beginning insulin treatment, there is often a temporary reduction in exogenous insulin demand. [44]
• Dosage should be adjusted according to glycemic monitoring.
This may need to be increased for
patients with obesity, those with low
insulin sensitivity, and patients
experiencing puberty.
This honeymoon period is due to a
temporary recovery of endogenous insulin
production of the pancreatic ß cells. The
autoimmune destruction of ß cells
progresses during the course of the
disease, causing the insulinrequirement to
increase after this short interval.
While intensive lifestyle modifications can improve glycemic control
and reduce the need for medication to achieve glycemic goals, most
patients will require medication to achieve their glycemic targets.
These recommendations are consistent with the 2024 ADA guidelines.
It reduces liver production of glucose, increases insulin sensitivity, and induces weight loss.
Includes severely impaired renal function (eGFR < 30 mL/minute/1.73 m2), acute or chronic metabolic acidosis (including diabetic ketoacidosis), and hypersensitivity to metformin or any of its components.
E.g., comorbidities, preferences,
risk for hypoglycemia
⑭
*
-
DPP-4 i
zin](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-14-2048.jpg)
![GLP-1 receptor agonists
Injectable
Other subcutaneous GLP-1 receptor
agonists
Daily liraglutide
Weekly dulaglutide
Recommended for patients with eGFR < 30 mL/min/1.73 m2
Consider in patients with clinical ASCVD, high risk of ASCVD.
Beneficial for patients who need to lose or maintain their weight
Sulfonylureas Glimepiride
Increases risk for hypoglycemia
Low cost
Thiazolidinedione Pioglitazone
Avoid in patients with congestive heart failure.
Low cost
Other drugs that are not part of the therapy algorithms for according to the ADA guideline include:
Meglitinides: e.g., nateglinide
Alpha-glucosidase inhibitors: acarbose
Amylin analogs: injectable pramlintide
See “Overview of antidiabetic drugs” for details on side effects and contraindications.
Indications for insulin therapy in T2DM
Patients whose glycemic targets are not met despite sufficient antidiabetic treatment
Patients with contraindications for noninsulin antidiabetic drugs, e.g., patients with end-stage renal failure
Pregestational and gestational diabetes
Hyperglycemic crisis
Consider in newly diagnosed patients with any of the following:
Initial glucose ≥ 300 mg/dL or > 10%
Signs of a continued catabolic state, e.g., weight loss
Approach to insulin treatment in
Start with the simplest insulin regime, i.e., a basal insulin regimen with once-daily injections.
Noninsulin antidiabetics may be continued when insulin treatment is started.
See “Insulin regimens” for details.
T2DM
Oral monotherapy usually lowers levels by ∼ 1%. Every noninsulin drug added to meaormin will lower the by an
additional ∼ 0.7–1.0%.
HbA1c HbA1c
[31]
Beware of drug interactions and drug incompatibilities; combining sulfonylureas with insulin increases the risk of hypoglycemia.
[46]
Many oral antidiabetic drugs should be avoided in patients undergoing surgery or experiencing severe illness. Instead, insulin
therapy may be initiated.
[31]
[47]
HbA1c
Symptoms of hyperglycemia
T2DM [31]
glutide
92D
metfo -y 6 % 1 Aba
S
salt-Zin
S
S DiPP4 : - Lipton
- GLP1-ygluxin
- So = -
-
T2D- Zone
I
2
3
4
E
A
·](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-15-2048.jpg)

![See “Insulin regimens” for details.
COLLAPSE NOTES FEEDBACK
Screening for complications of diabetes
Screening for microvascular complications of diabetes
Initial screening
: 5 years aAer the onset of diabetes
: at the time of
Frequency
Perform at minimum every 12 months.
More frequent screening may be necessary for:
Pregnant patients
Patients with a history of microvascular complications
Modalities
Screening for diabetic kidney disease: spot urine albumin to creatinine ratio (UACR) and serum glomerular filtration rate
Screening for diabetic retinopathy: comprehensive eye exam with dilation or retinal photography (if available)
Screening for diabetic peripheral neuropathy with a focused examination of sensation, e.g.:
Monofilament test
Pinprick sensation or temperature sensation
Vibration sense (using a tuning fork)
Screening for diabetic autonomic neuropathy by recording resting heart rate, orthostatic vital signs, and heart rate variability.
Screening for diabetic foot: comprehensive foot exam
Screening for macrovascular complications of diabetes
Check BP at every clinic appointment and encourage patients with elevated BP to measure blood pressure at home.
Obtain a lipid panel at the time of and repeat every 5 years for patients < 40 years.
Screening for cardiovascular disease is not recommended for asymptomatic individuals.
GLP-1 receptor agonists should be part of the treatment strategy prior to starting insulin treatment in patients with , unless
they are not appropriate or insulin therapy is preferred.
T2DM
If treatment goals are not met in a patient on a basal insulin regimen, combination therapy with basal insulin and injectable GLP-1
receptor agonists may be considered.
[48][49][50]
Type 1 DM [51]
Type 2 DM diabetes diagnosis
[48][49][50]
[50][51]
[49]
[49][51]
[49][52][53]
[54]
diabetes diagnosis
[34]
High-quality images of the
fundus can be obtained with
retinal photography and
reviewed remotely by
ophthalmic specialists. A follow-
up eye exam is indicated if the
images are abnormal or of poor
quality.
For evaluation of small nerve fibers
For evaluation of large nerve fibers
Home BP measurements
appear to correlate
better with ASCVD risk
than BP measurements
taken in healthcare
settings.
After age 40, all patients with diabetes are
recommended to take a statin for ASCVD
prevention regardless of lipid levels.
·](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-17-2048.jpg)
![Screening for cardiovascular disease is not recommended for asymptomatic individuals.
COLLAPSE NOTES FEEDBACK
Complications
Acute complications
Hyperglycemic crisis: undiagnosed or insufficiently treated diabetes mellitus may result in severe , potentially culminating in a crisis
Hyperosmolar hyperglycemic state (HHS)
Diabetic ketoacidosis (DKA)
Life-threatening hypoglycemia: secondary to inappropriate insulin therapy
Long-term complications
Macrovascular disease (atherosclerosis)
Prevalence: more common in patients with
Risk factors: The major determinants are metabolic risk factors, which include obesity, dyslipidemia, and arterial hypertension. may
be less related to the development of macrovascular disease.
Manifestations
Coronary heart disease (most common cause of death)
Cerebrovascular disease
Peripheral artery disease (possible loss of limb)
Monckeberg arteriosclerosis
Gangrene
Microvascular disease
Onset: typically arises 5–10 years aQer onset of disease
Pathophysiology: chronic → nonenzymatic glycation of proteins and lipids → thickening of the basal membrane with progressive
function impairment and tissue damage
Manifestations
Diabetic nephropathy
Diabetic retinopathy, glaucoma
Diabetic neuropathy including diabetic gastroparesis
Diabetic foot
[34]
hyperglycemia
[55]
type 2 diabetes
Hyperglycemia
hyperglycemia
Strict glycemic control is crucial in preventing microvascular disease.
Both forms of diabetes eventually lead to microvascular and macrovascularcomplications.
A form of arteriosclerosis characterized by calcification of the media and internal elastic lamina that do not cause arterial stenosis. It
is associated with diabetes mellitus and/or progressive kidney disease and usually affects arteries in the extremities.](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-18-2048.jpg)
![Necrobiosis lipoidica
Definition: inflammatory granulomatous disorder of the skin; characterized by collagen degeneration and lipid accumulation in the surface of the
skin.
Epidemiology
> 60% association with DM
♀
>>
♂
Clinical features
Rash: circumscribed, erythematous plaques with atrophic centers and irregular margins
Common sites: pretibial region
Usually asymptomatic
Ulcerations with subsequent scarring may occur.
Histopathology: necrobiotic palisading granuloma
Lymphohistiocytic infiltration with plasma cells, foam cells, and giant cells
Wall thickening and occlusion of small blood vessels
Destruction of collagen fibers in the entire corium
Treatment: Corticosteroids may be effective (e.g., intralesional corticosteroid injections).
Other complications
Mucormycosis (zygomycosis)
Diabetic cardiomyopathy: a disorder of the myocardium seen in patients with diabetes
Chronic results in altered metabolism of glucose and faOy acids, microangiopathy with endothelial dysfunction, and autonomic
neuropathy, which collectively results in cardiomyocyte hypertrophy, myocardial fibrosis, ventricular dilation, and ultimately in systolic and/or
diastolic heart failure.
This disorder may or may not be accompanied by CVD and hypertension.
Osmotic damage: occurs in tissues with high aldolase reductase activity and low/absent sorbitol dehydrogenase activity (e.g., eyes, peripheral
nerves) → cataracts, neuropathy
Diabetic faOy liver disease
Hyporeninemic hypoaldosteronism
Hypoaldosteronism that is caused by decreased renin activity
Most commonly caused by diabetic nephropathy or chronic interstitial nephritis
Patients present with features of hypoaldosteronism, i.e., hypotension, hyponatremia, and type 4 renal tubular acidosis.
Limited joint mobility syndrome (formerly known as diabetic )
Manifested as stiffness of the small joints of the hand
[56]
Candidal intertrigo Necrobiosis lipoidica Necrobiosis lipoidica Necrobiosis lipoidica
[57]
hyperglycemia
[58]
cheiroarthropathy [59]
Disease affects < 1% of patients with diabetes.
I 234
& 2 3 4](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-19-2048.jpg)
![Tight waxy skin, particularly on the dorsal surface of the fingers, is common.
Positive prayer sign: inability to approximate the palms due to flexion contractures of the PIP and MCP joints
Positive tabletop test: inability to flaCen the palm against the surface of a table due to the contractures in the metacarpophalangeal joints
Sialadenosis
Increased risk of infection
We list the most important complications. The selection is not exhaustive.
COLLAPSE NOTES FEEDBACK
Prognosis
Diabetes mellitus is one of the leading causes of death in the US; common complications that result in death are myocardial infarction and end
stage renal failure.
One of the leading causes of blindness, nontraumatic lower limb amputation, end stage renal failure, and cardiovascular disease
The prognosis primarily depends on glycemic control and treatment of comorbidities (e.g., hypertension, dyslipidemia).
COLLAPSE NOTES FEEDBACK
[60]
Carbuncle Positive prayer sign
[4]
[4]
Poor perfusion of tissue (macrovascular/microvascular disease) and a weak immune system may lead to a higher risk of infection.
In addition, growth of bacteria and fungi (e.g., Candida albicans) occurs, likely due to hyperglycemia. Certain infections occur
almost exclusively in patients with diabetes (e.g., otitis externamaligna due to Pseudomonas aeruginosa).](https://image.slidesharecdn.com/diabetesmellitus-amboss-250827083429-6488174f/75/Diabetes-mellitus-AMBOSS-pdf-20-2048.jpg)



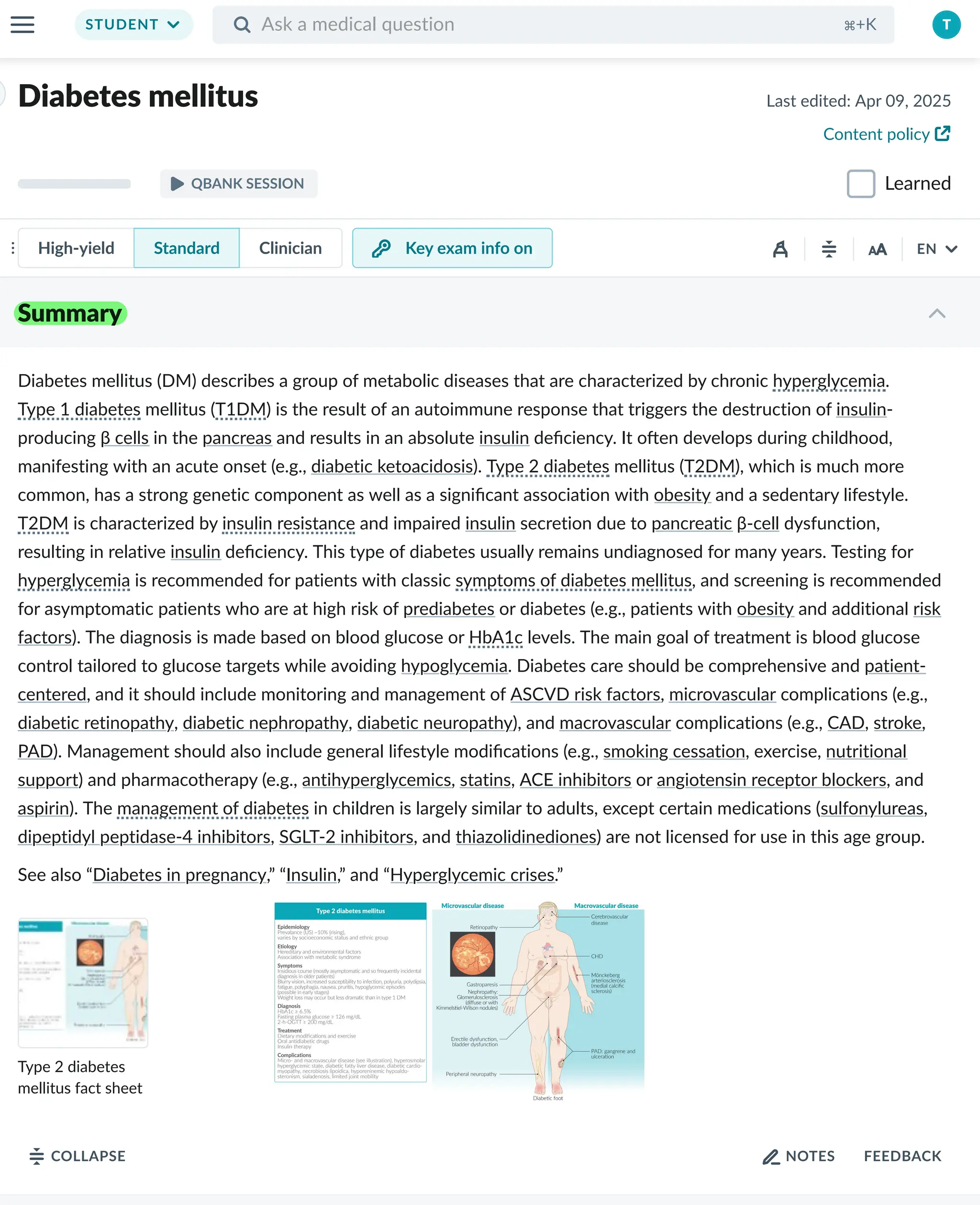
Diabetes mellitus (DM) describes a group of metabolic diseases that are characterized by chronic . hyperglycemia Type 1 diabetes T1DM mellitus ( ) is the result of an autoimmune response that triggers the destruction of insulin- producing β cells in the pancreas and results in an absolute insulin deficiency. It oHen develops during childhood, manifesting with an acute onset (e.g., diabetic ketoacidosis). Type 2 diabetes T2DM mellitus ( ), which is much more common, has a strong genetic component as well as a significant association with obesity and a sedentary lifestyle. T2DM insulin resistance is characterized by and impaired insulin secretion due to pancreatic β-cell dysfunction, resulting in relative insulin deficiency. This type of diabetes usually remains undiagnosed for many years. Testing for hyperglycemia is recommended for patients with classic symptoms of diabetes mellitus , and screening is recommended for asymptomatic patients who are at high risk of prediabetes or diabetes (e.g., patients with obesity and additional risk factors). The diagnosis is made based on blood glucose or HbA1c levels. The main goal of treatment is blood glucose control tailored to glucose targets while avoiding hypoglycemia. Diabetes care should be comprehensive and patient- centered, and it should include monitoring and management of ASCVD risk factors, microvascular complications (e.g., diabetic retinopathy, diabetic nephropathy, diabetic neuropathy), and macrovascular complications (e.g., CAD, stroke, PAD). Management should also include general lifestyle modifications (e.g., smoking cessation, exercise, nutritional support) and pharmacotherapy (e.g., antihyperglycemics, statins, ACE inhibitors or angiotensin receptor blockers, and aspirin). The management of diabetes in children is largely similar to adults, except certain medications (sulfonylureas, dipeptidyl peptidase-4 inhibitors, SGLT-2 inhibitors, and thiazolidinediones) are not licensed for use in this age group. See also “Diabetes in pregnancy,” “Insulin,” and “Hyperglycemic crises.”







































![DM lecture for c1 [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/dmlectureforc1autosaved-220720190831-86418752-thumbnail.jpg?width=640&height=640&fit=bounds)







































