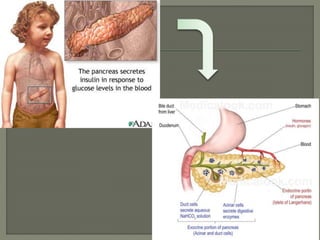
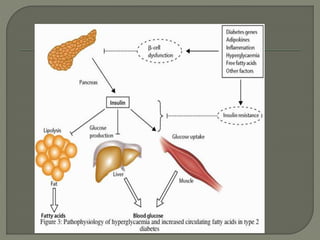
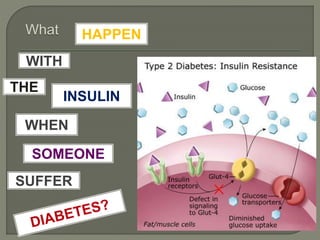
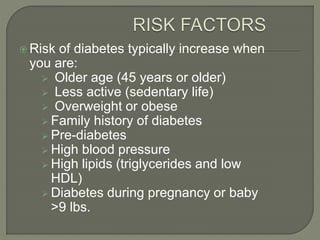
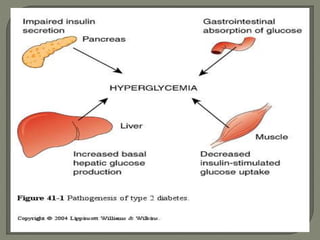
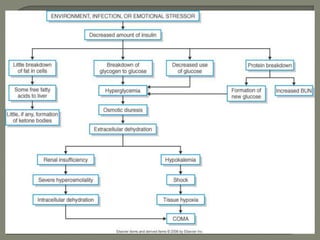
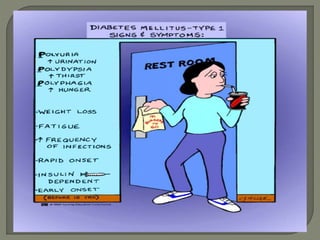
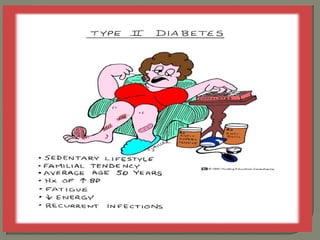
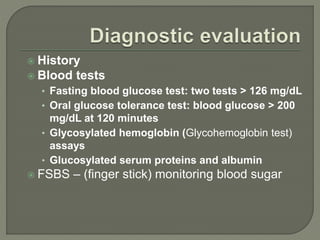
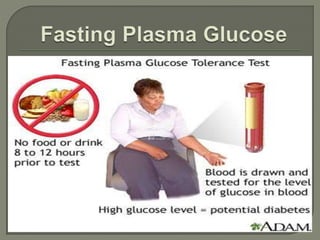
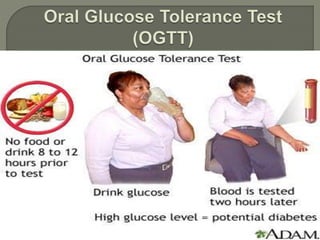
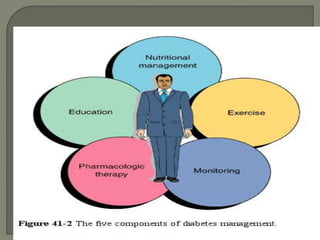
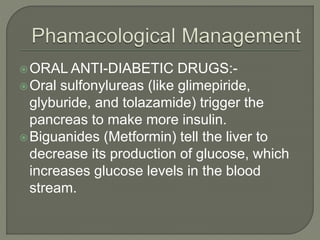
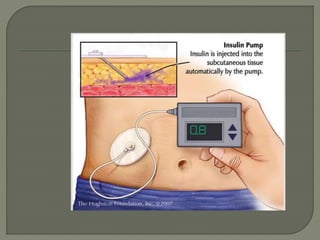
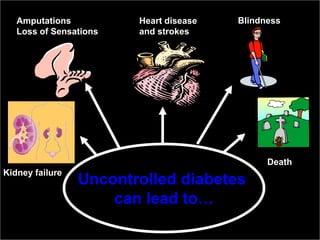
This document discusses diabetes mellitus, a metabolic disorder characterized by high blood sugar levels resulting from defects in insulin production or insulin action. There are three main types of diabetes: type 1 caused by lack of insulin production; type 2 caused by insulin resistance; and gestational diabetes during pregnancy. Risk factors include family history, age, obesity, and physical inactivity. Symptoms include frequent urination, increased thirst and hunger. Diagnosis involves blood and urine tests. Treatment depends on diabetes type but may include medications to increase insulin production/sensitivity, insulin injections, diet control, exercise, blood sugar monitoring and management of complications which can include kidney disease, vision loss and heart disease if uncontrolled.