CONTENTS
INTRODUCTION
DEVELOPMENT OF MANDIBLE
PRENATALDEVELOPMENT OF MANDIBLE
POSTNATAL DEVELOPMENT OF MANDIBLE
BLOOD SUPPLY
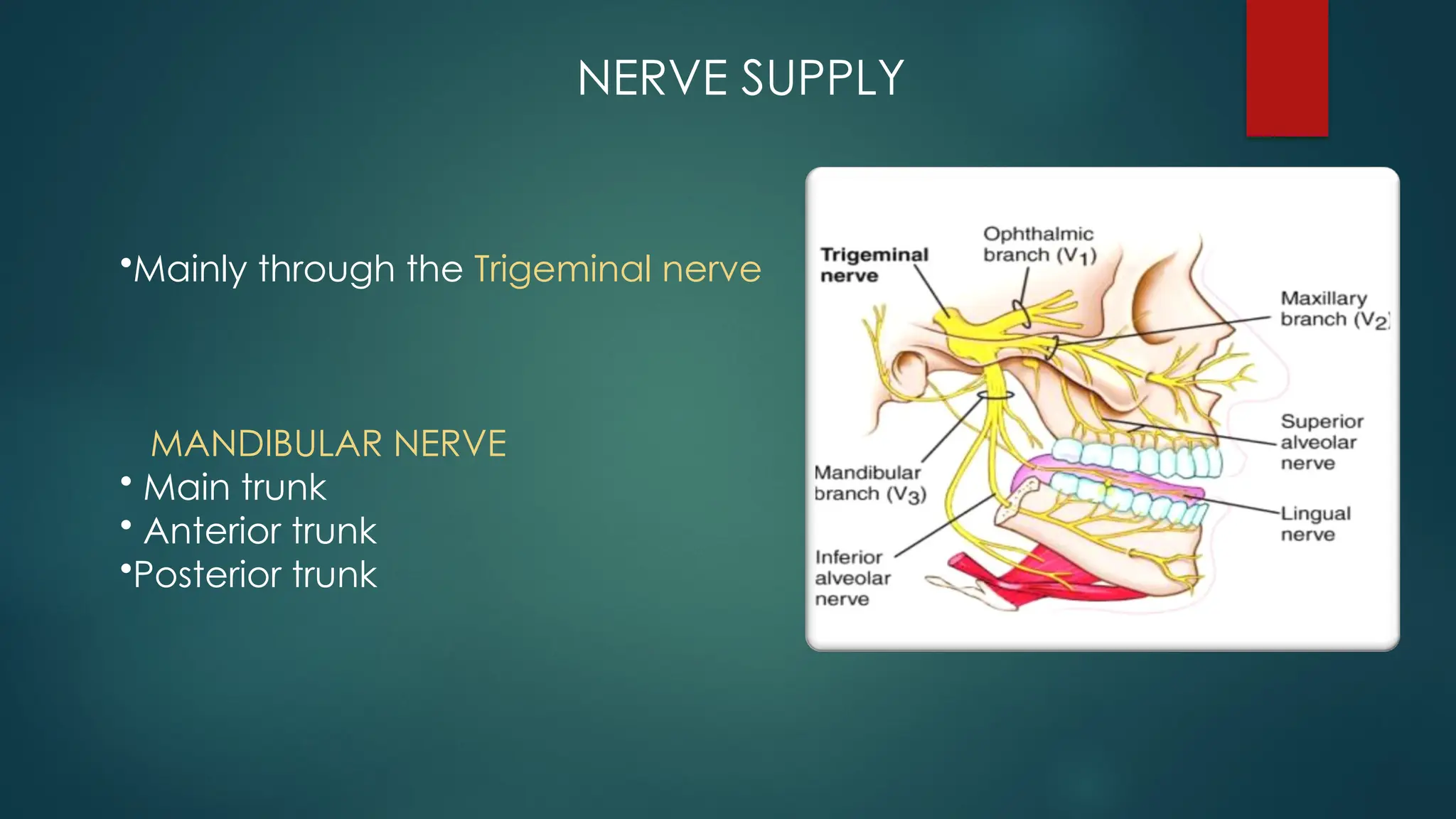
NERVE SUPPLE
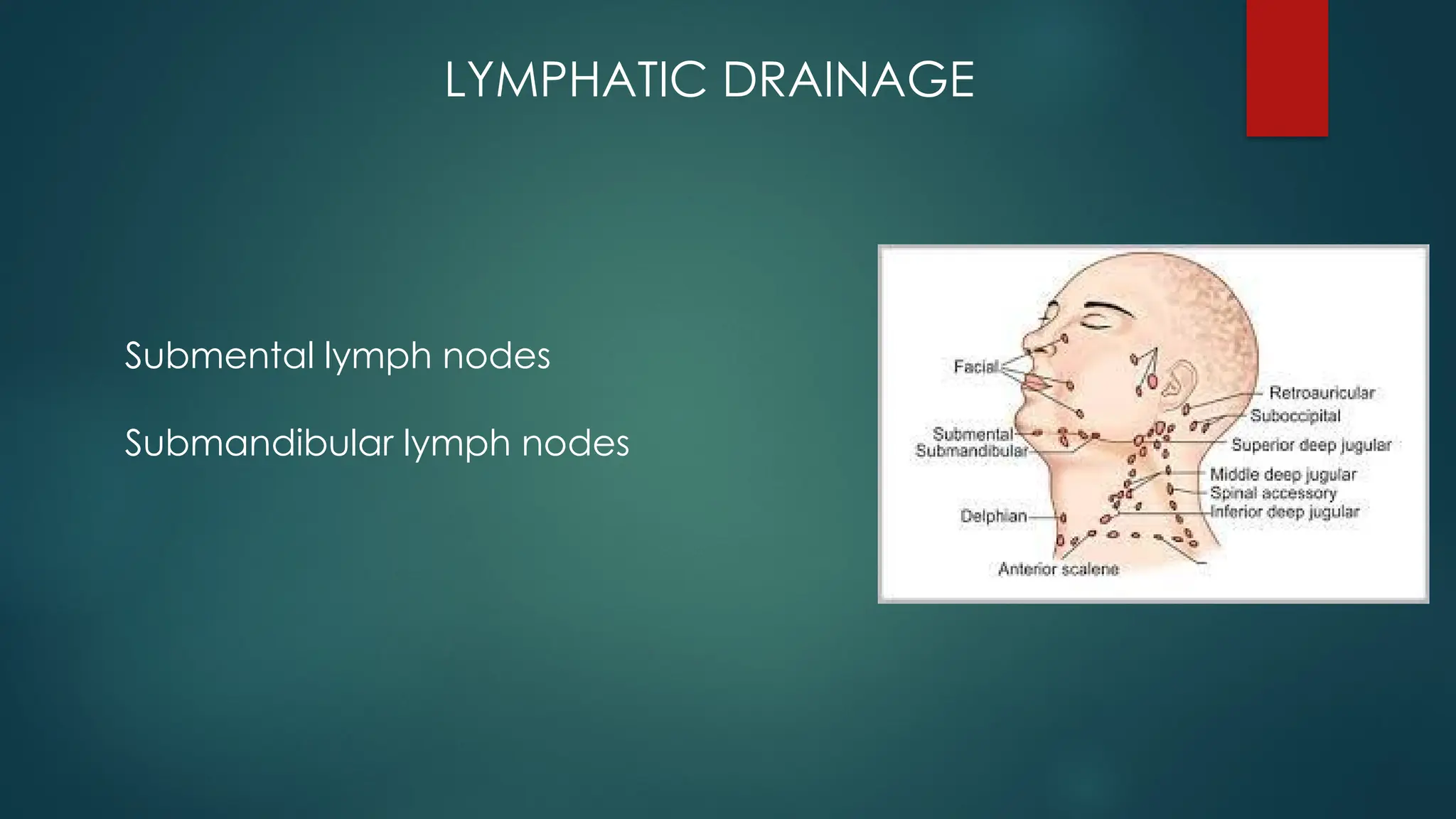
LYMPHATIC DRAINAGE
PHYSIOLOGICAL VARIANTS
AGE CHANGES
APPLIED ANATOMY
CONCLUSION
REFERENCES
3.
INTRODUCTION
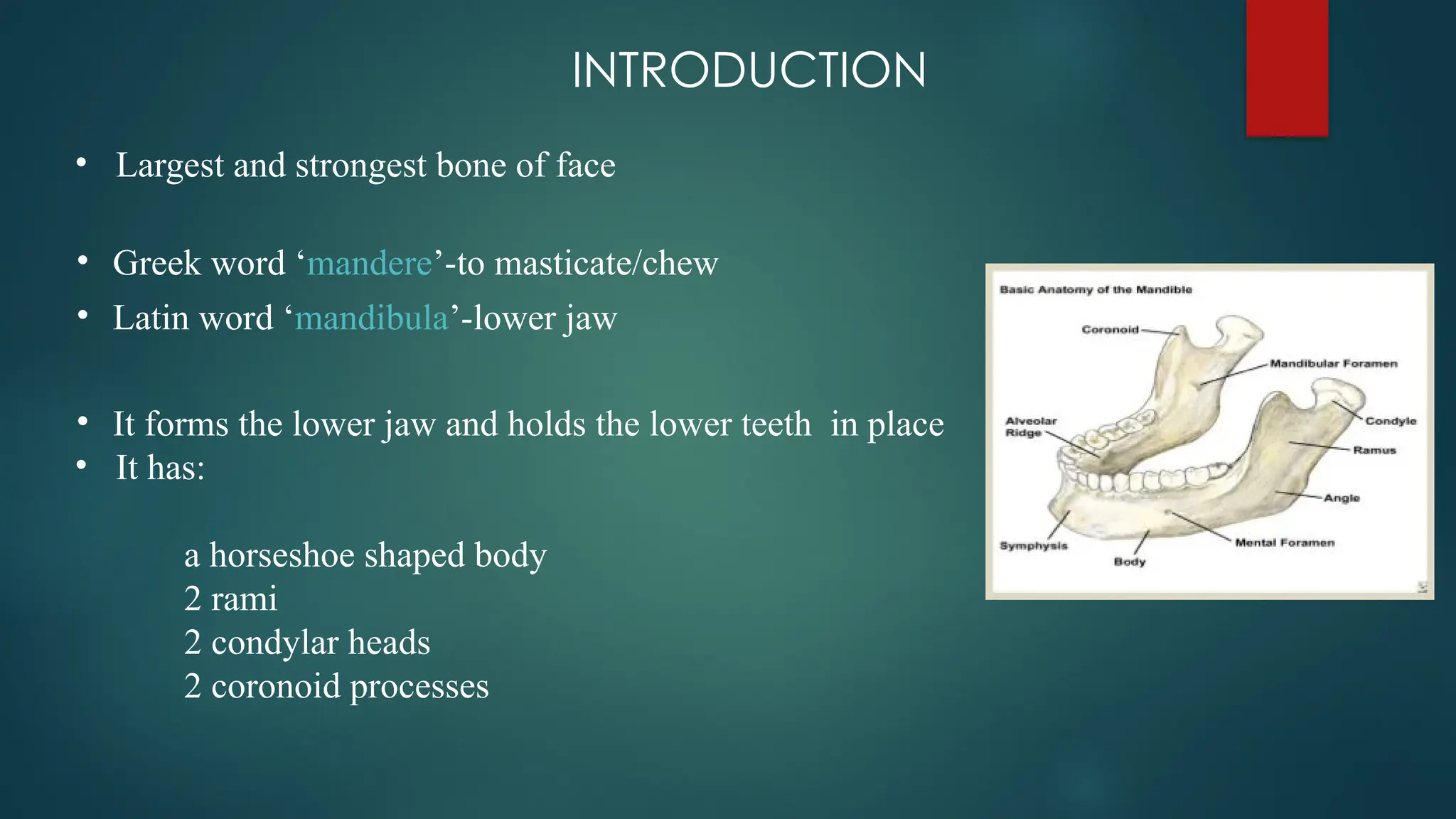
• Largest andstrongest bone of face
• Greek word ‘mandere’-to masticate/chew
• Latin word ‘mandibula’-lower jaw
• It forms the lower jaw and holds the lower teeth in place
• It has:
a horseshoe shaped body
2 rami
2 condylar heads
2 coronoid processes
4.
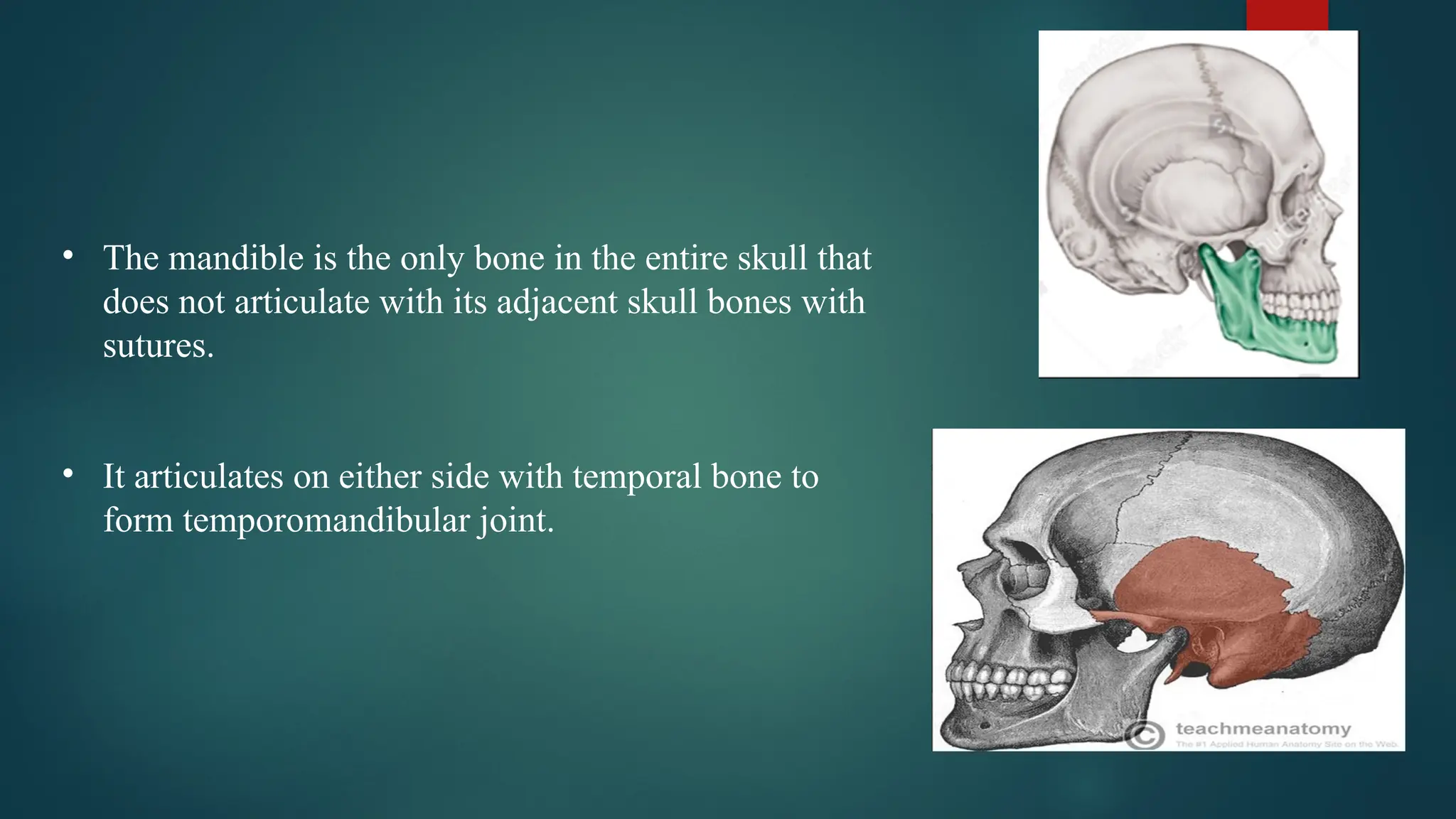
• The mandibleis the only bone in the entire skull that
does not articulate with its adjacent skull bones with
sutures.
• It articulates on either side with temporal bone to
form temporomandibular joint.
5.
DEVELOPMENT OF MANDIBLE
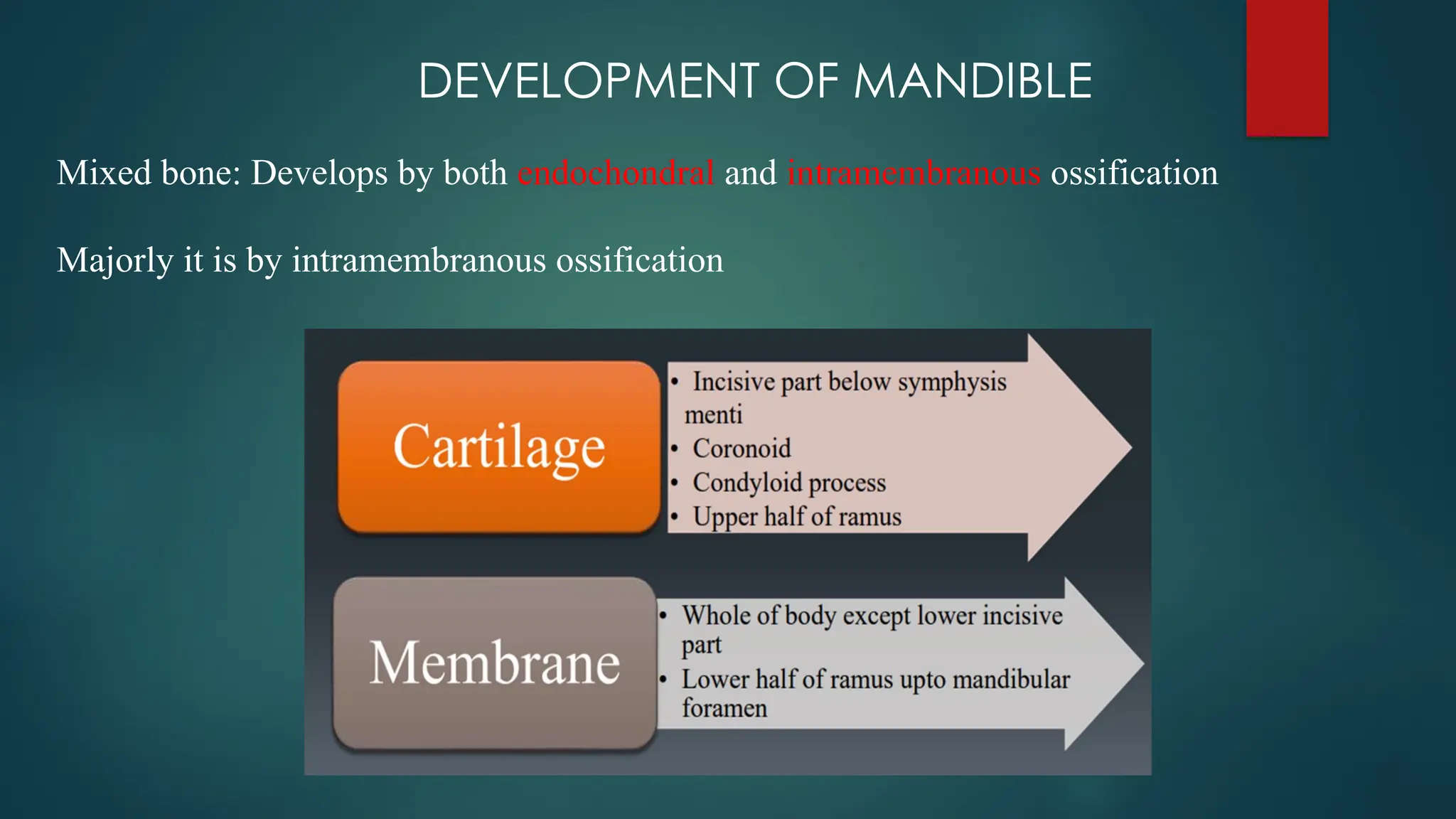
Mixedbone: Develops by both endochondral and intramembranous ossification
Majorly it is by intramembranous ossification
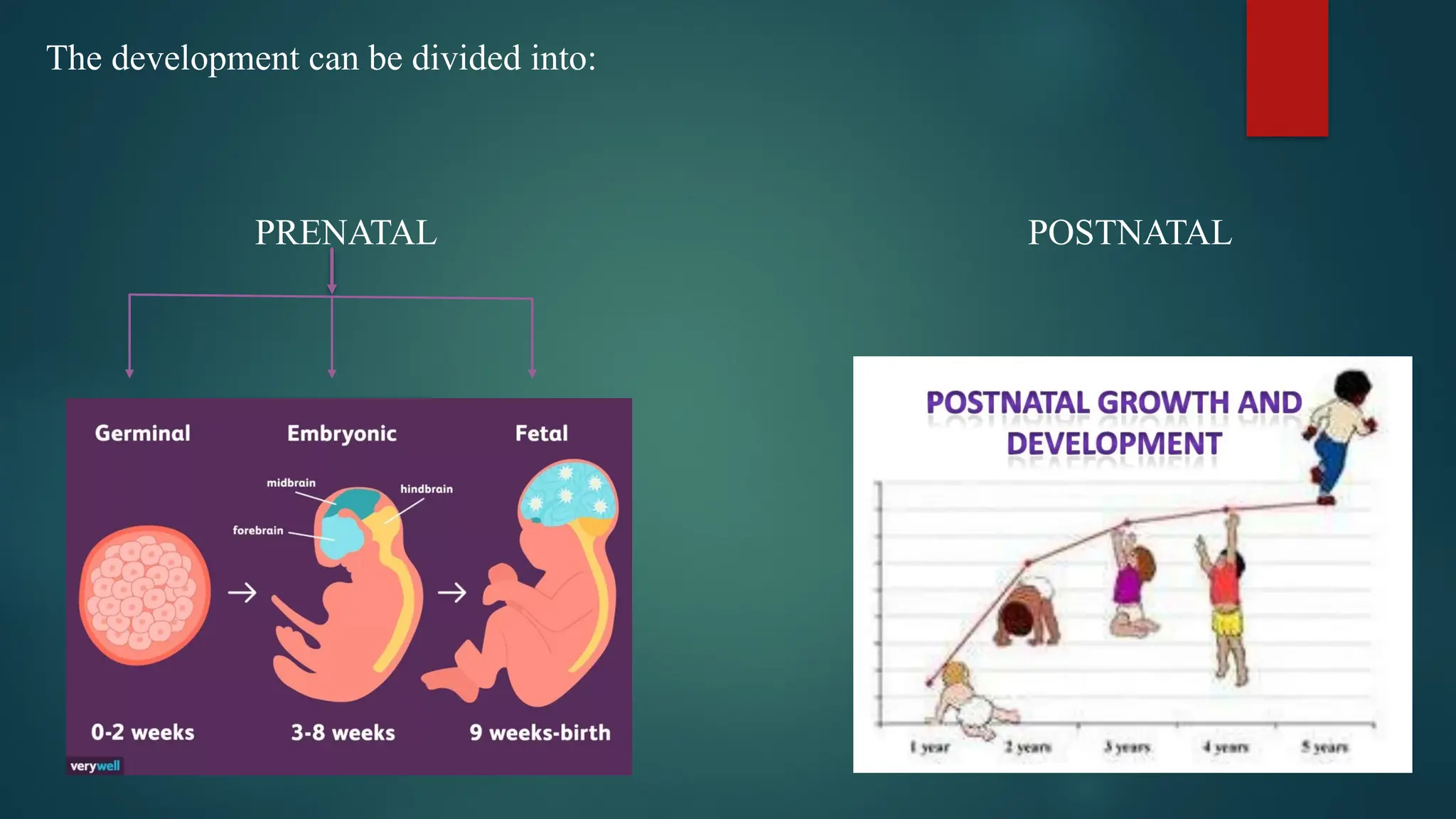
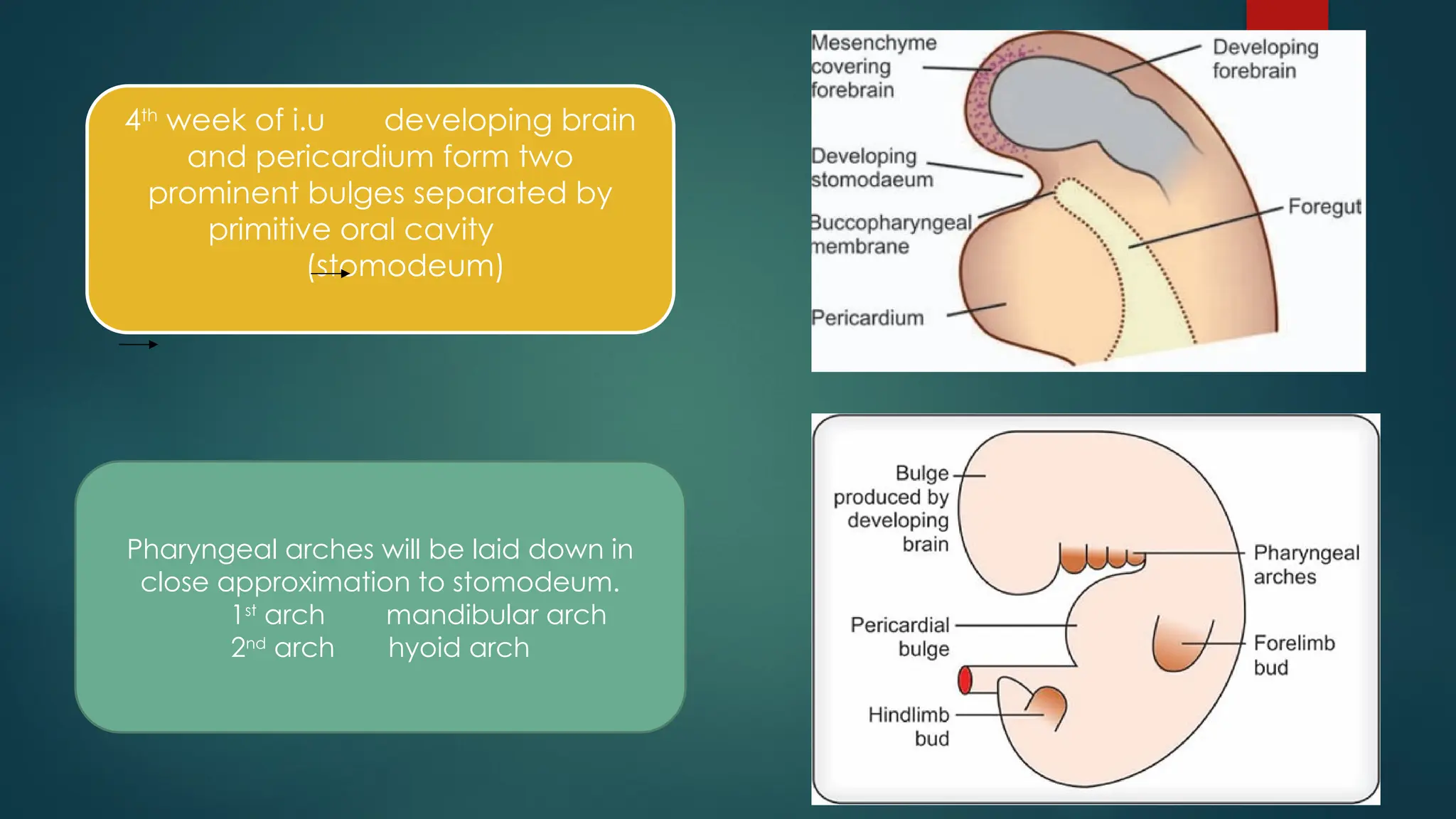
4th
week of i.udeveloping brain
and pericardium form two
prominent bulges separated by
primitive oral cavity
(stomodeum)
Pharyngeal arches will be laid down in
close approximation to stomodeum.
1st
arch mandibular arch
2nd
arch hyoid arch
8.
PRENATAL DEVELOPMENT OFMANDIBLE
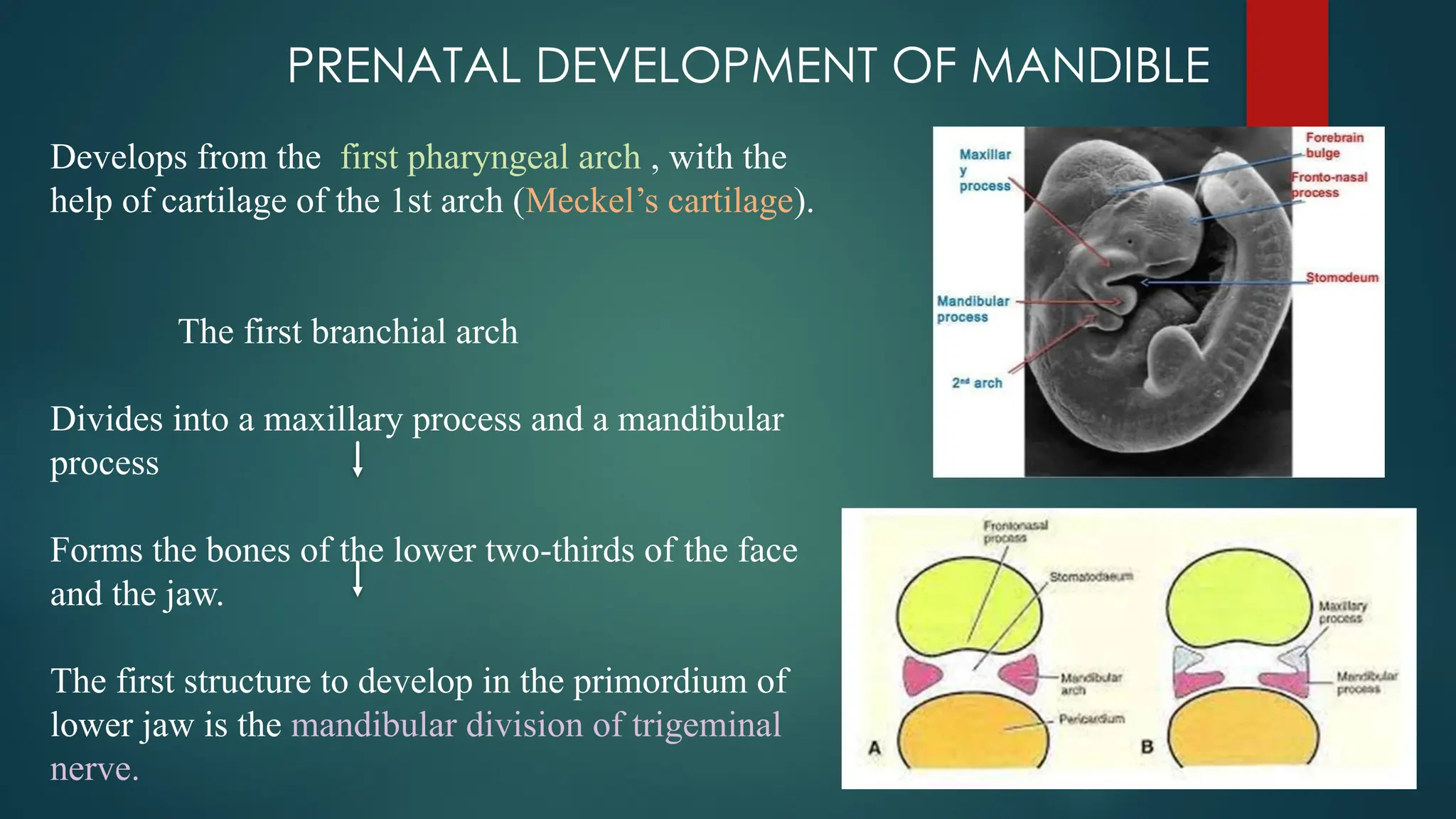
Develops from the first pharyngeal arch , with the
help of cartilage of the 1st arch (Meckel’s cartilage).
The first branchial arch
Divides into a maxillary process and a mandibular
process
Forms the bones of the lower two-thirds of the face
and the jaw.
The first structure to develop in the primordium of
lower jaw is the mandibular division of trigeminal
nerve.
9.
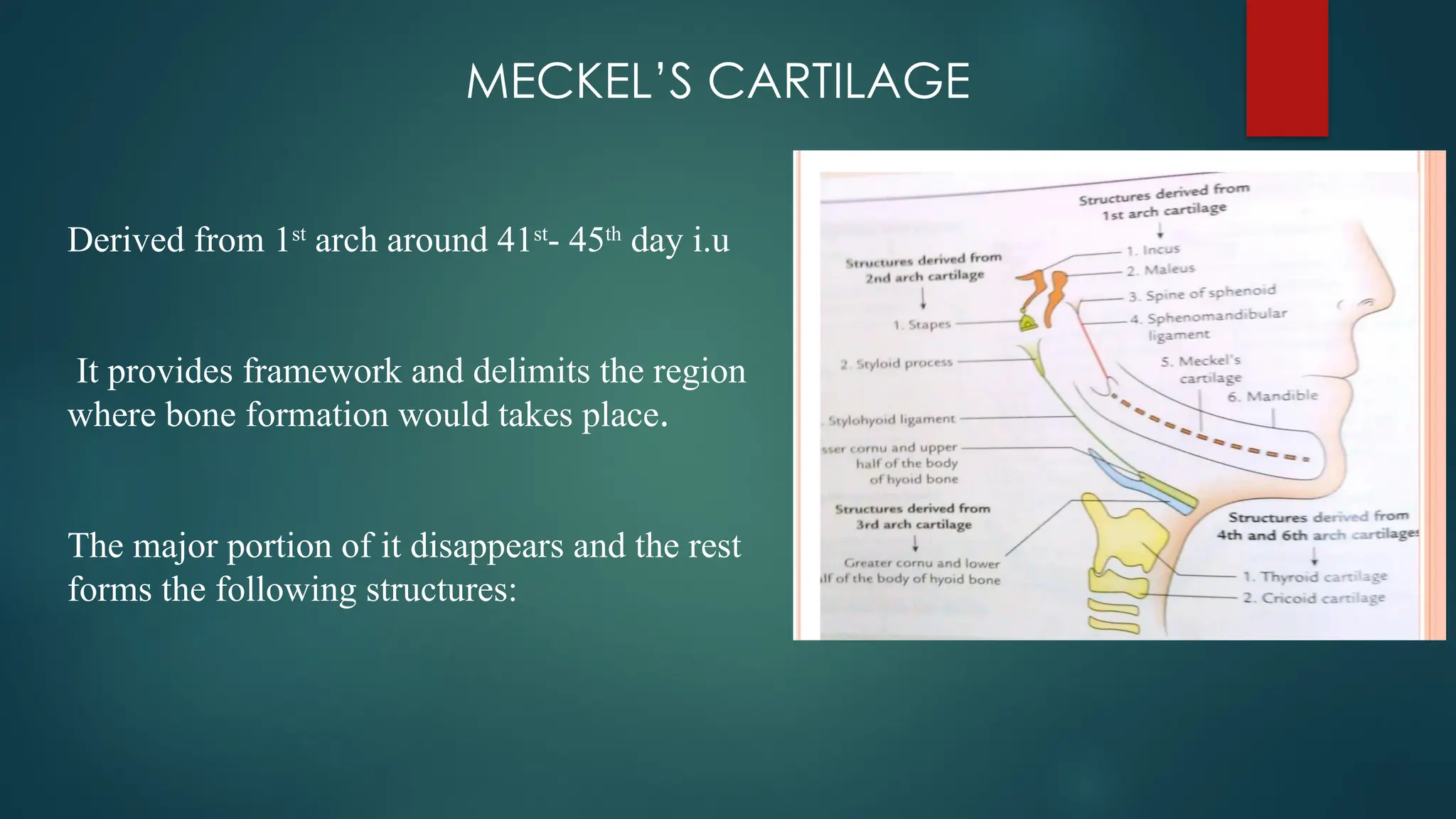
MECKEL’S CARTILAGE
Derived from1st
arch around 41st
- 45th
day i.u
It provides framework and delimits the region
where bone formation would takes place.
The major portion of it disappears and the rest
forms the following structures:
10.
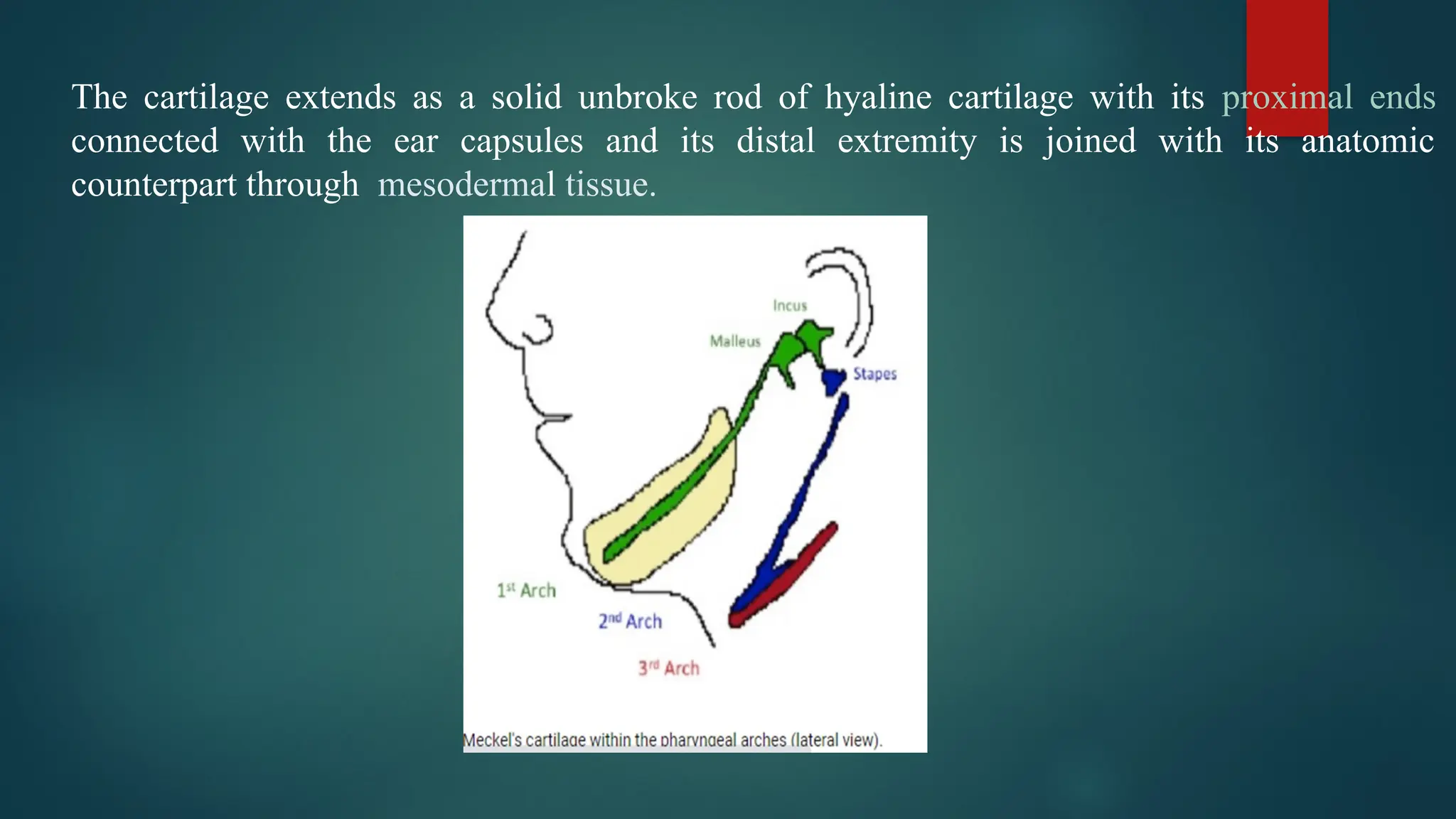
The cartilage extendsas a solid unbroke rod of hyaline cartilage with its proximal ends
connected with the ear capsules and its distal extremity is joined with its anatomic
counterpart through mesodermal tissue.
11.
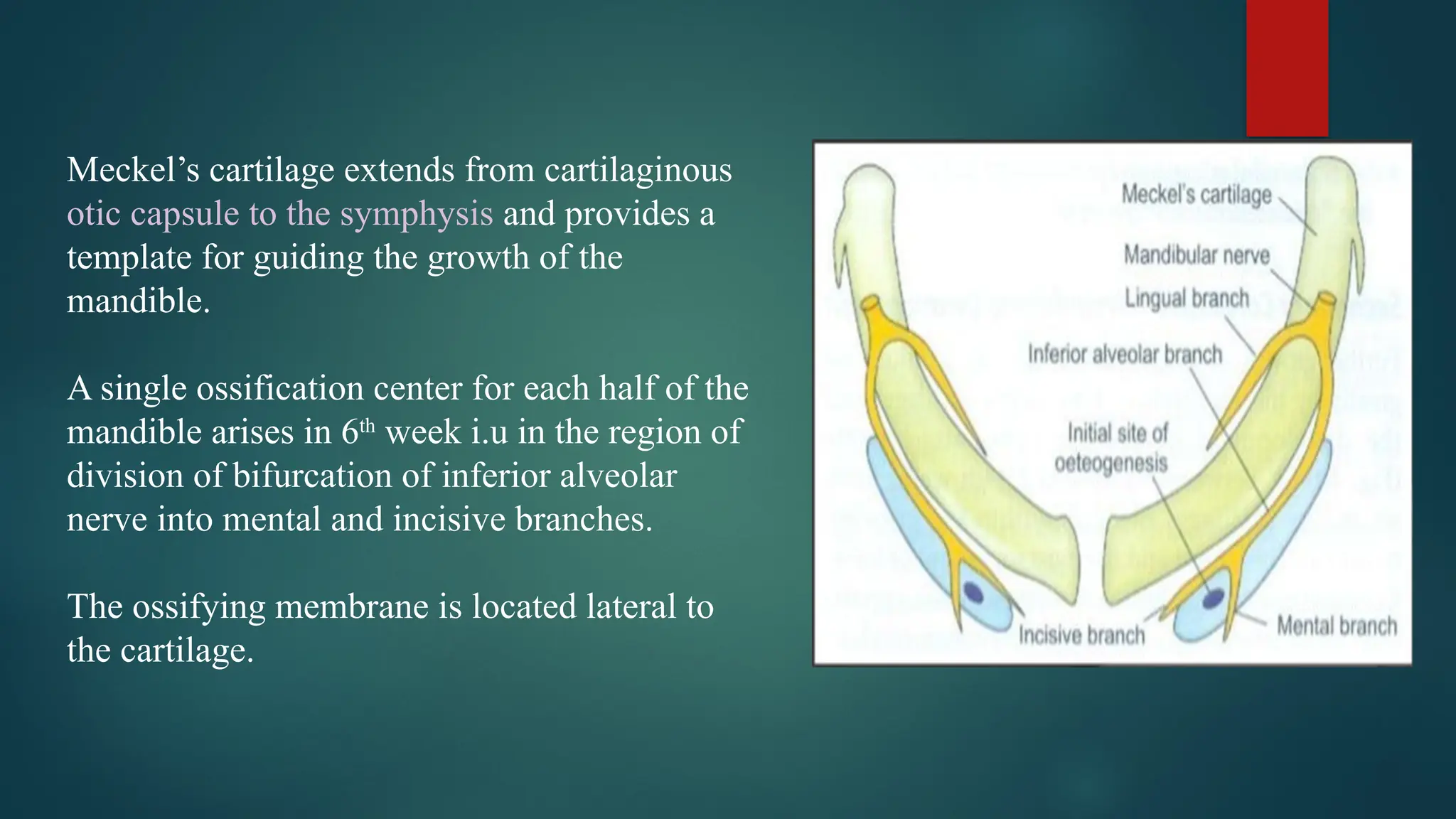
Meckel’s cartilage extendsfrom cartilaginous
otic capsule to the symphysis and provides a
template for guiding the growth of the
mandible.
A single ossification center for each half of the
mandible arises in 6th
week i.u in the region of
division of bifurcation of inferior alveolar
nerve into mental and incisive branches.
The ossifying membrane is located lateral to
the cartilage.
12.
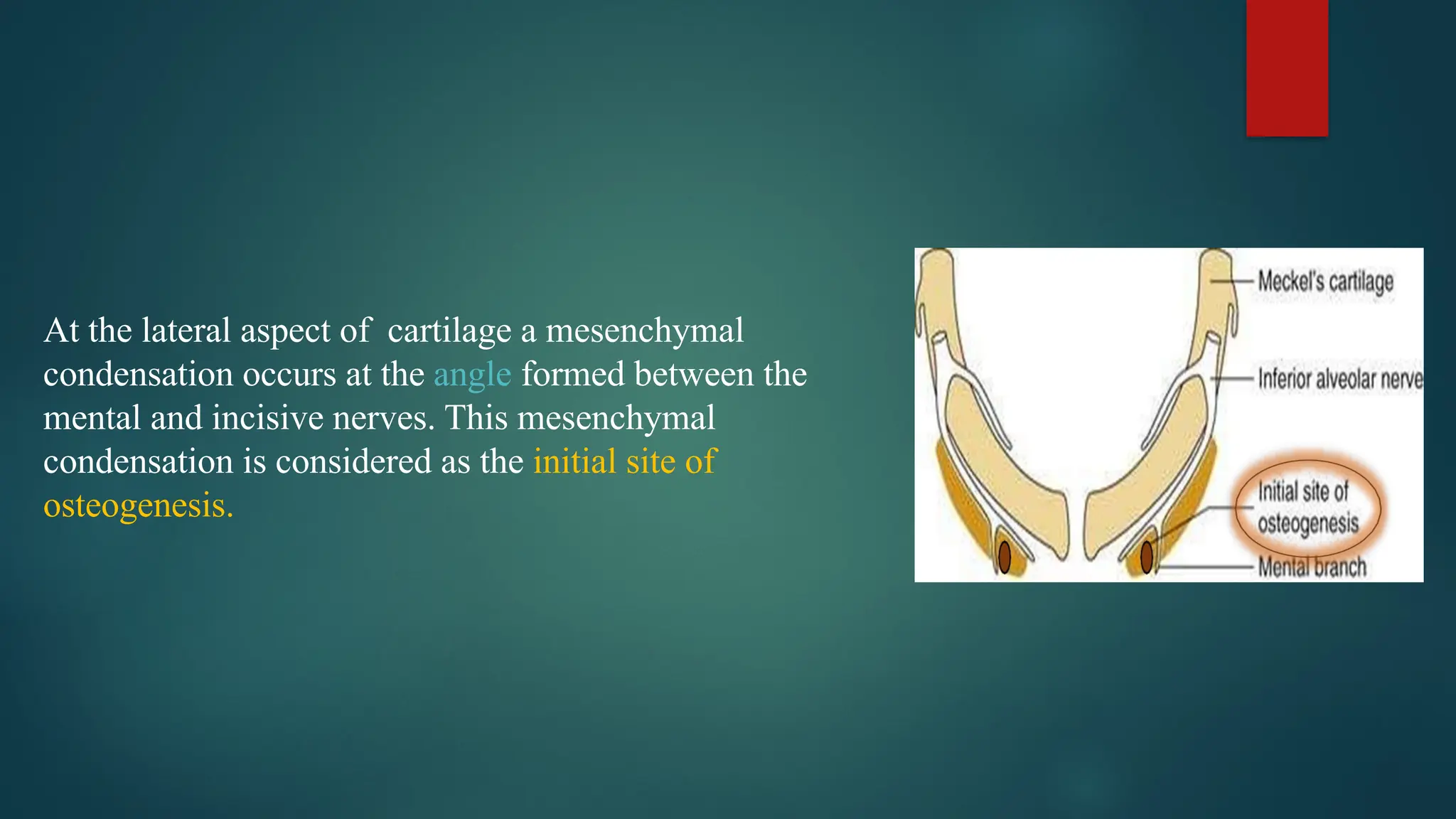
At the lateralaspect of cartilage a mesenchymal
condensation occurs at the angle formed between the
mental and incisive nerves. This mesenchymal
condensation is considered as the initial site of
osteogenesis.
13.
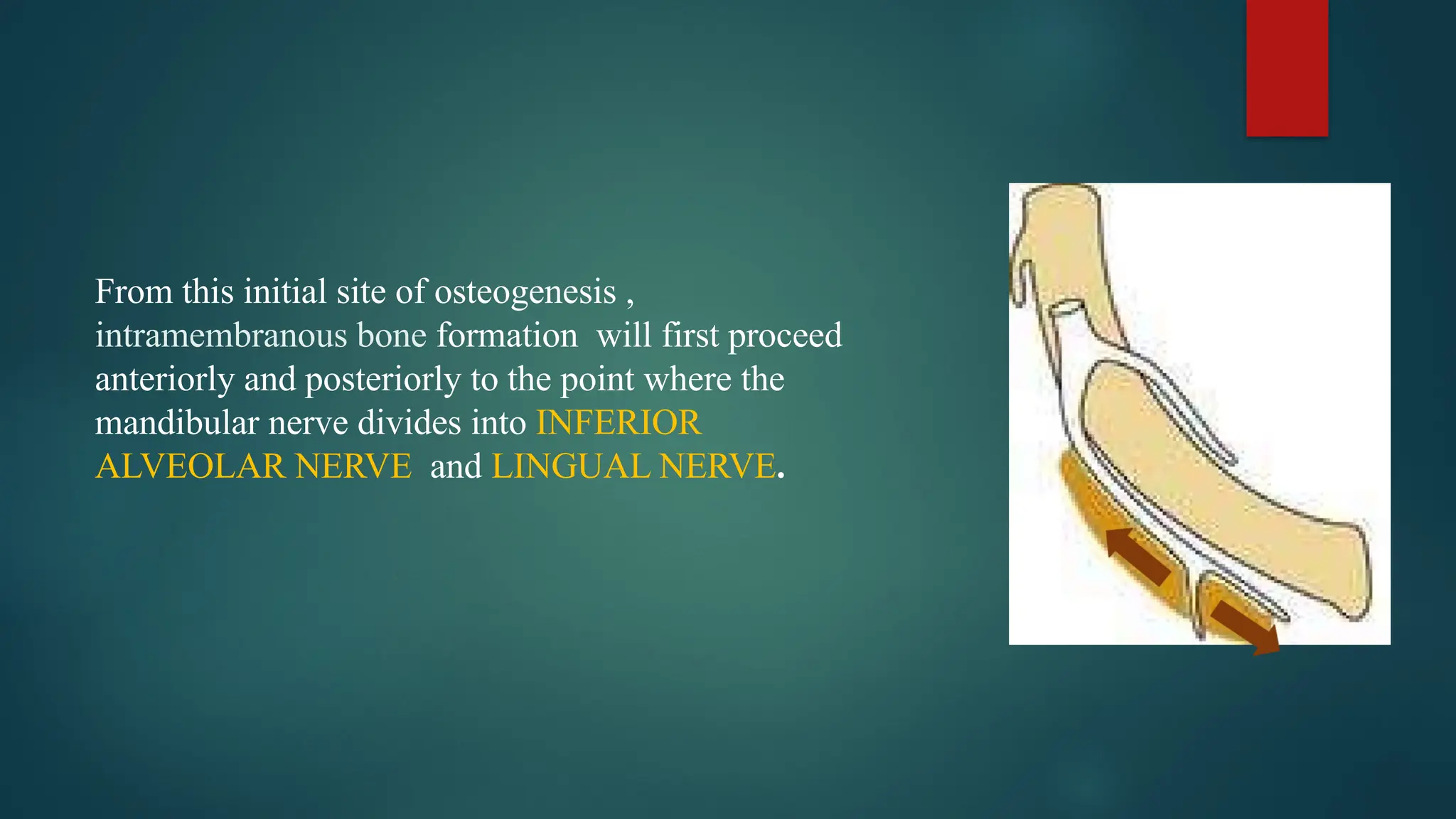
From this initialsite of osteogenesis ,
intramembranous bone formation will first proceed
anteriorly and posteriorly to the point where the
mandibular nerve divides into INFERIOR
ALVEOLAR NERVE and LINGUAL NERVE.
14.
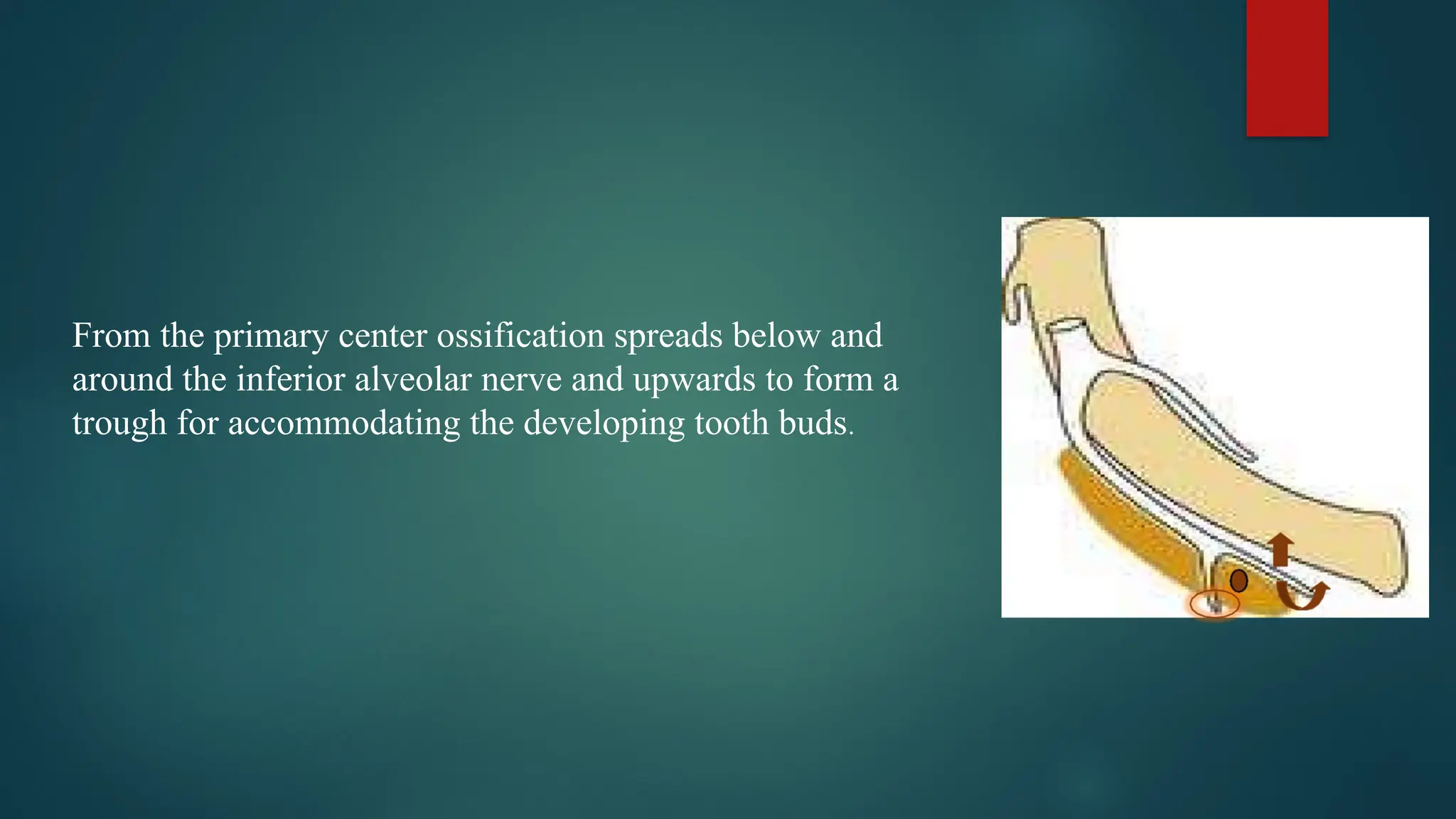
From the primarycenter ossification spreads below and
around the inferior alveolar nerve and upwards to form a
trough for accommodating the developing tooth buds.
15.
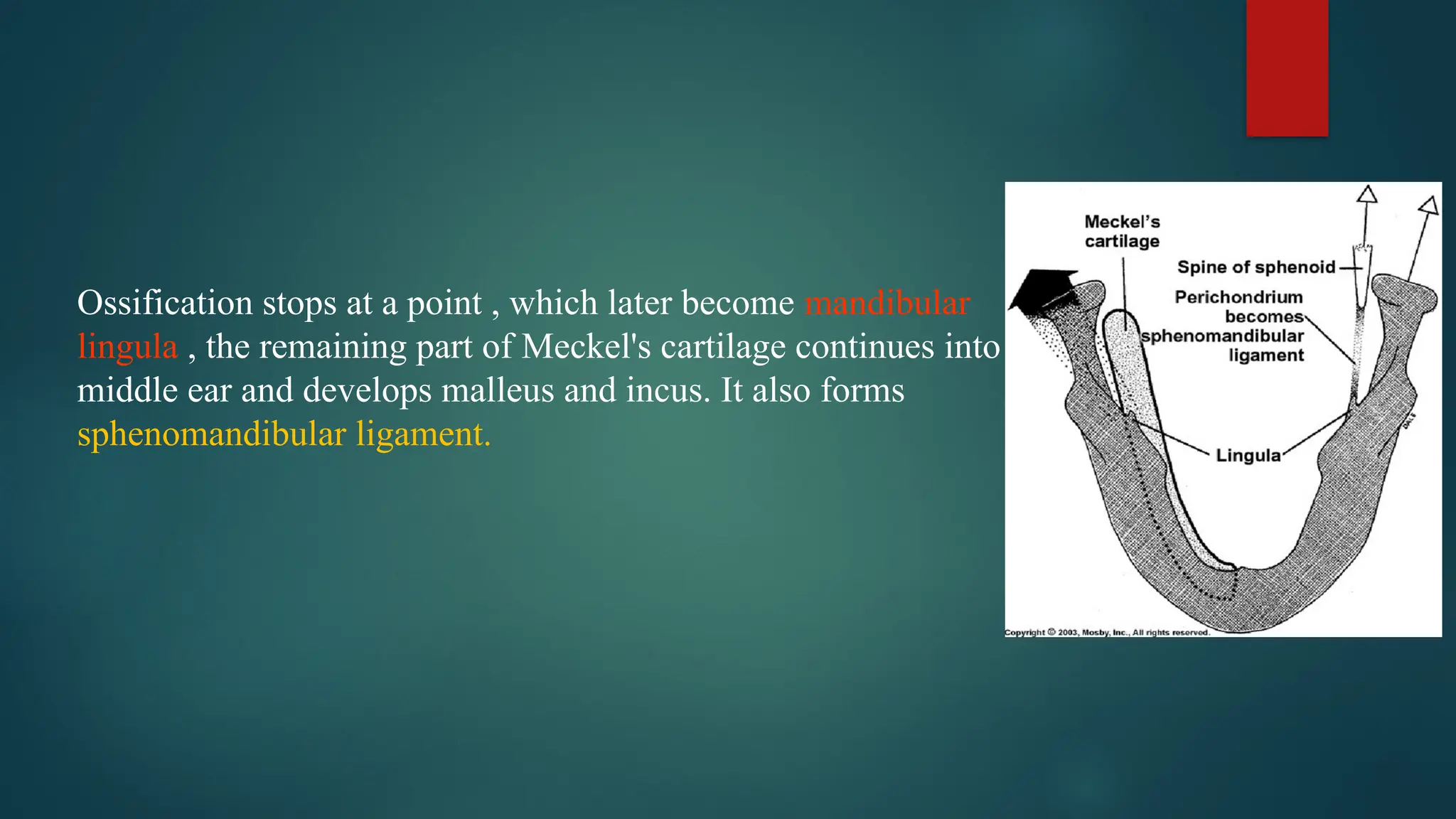
Ossification stops ata point , which later become mandibular
lingula , the remaining part of Meckel's cartilage continues into
middle ear and develops malleus and incus. It also forms
sphenomandibular ligament.
16.
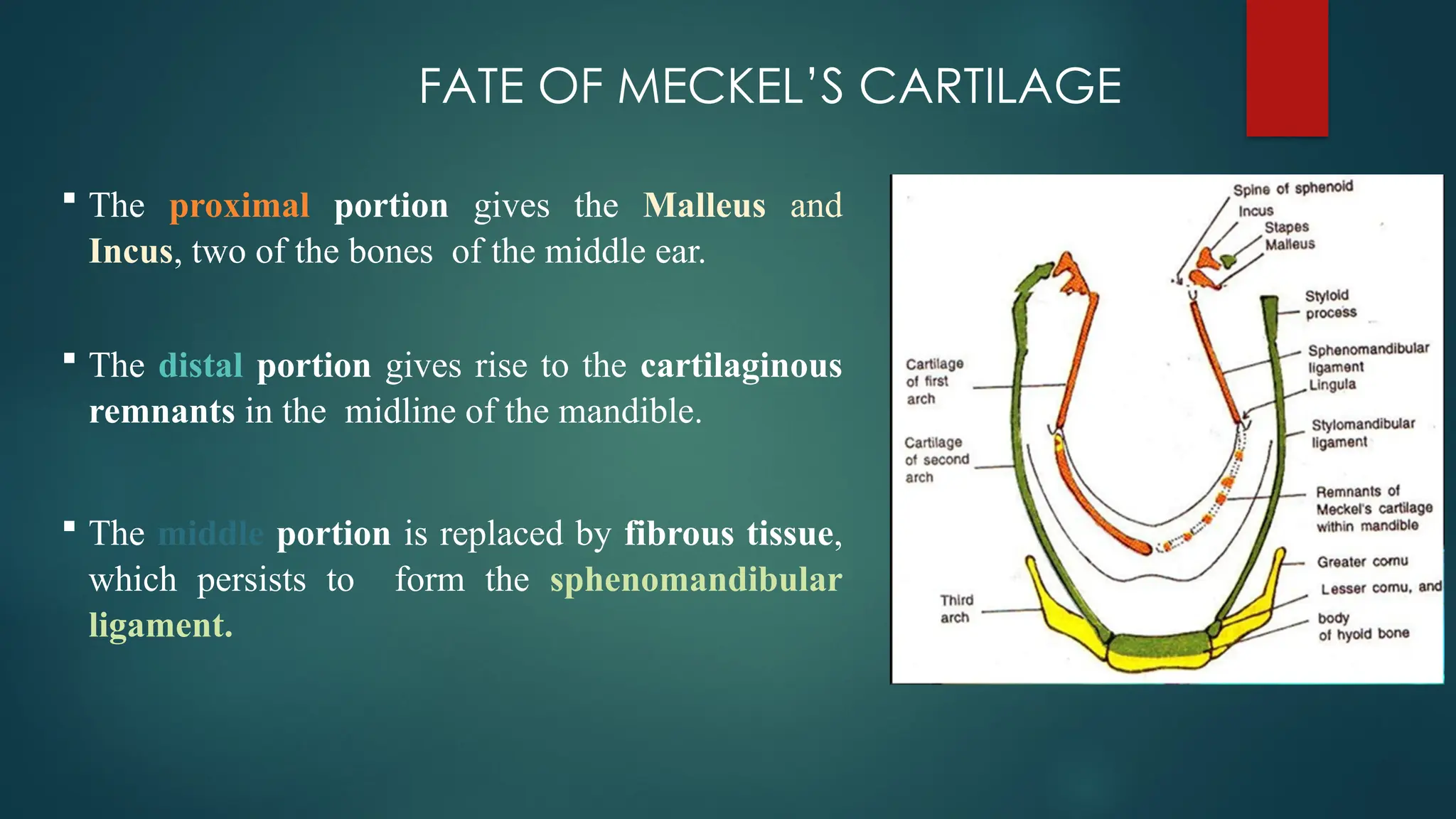
FATE OF MECKEL’SCARTILAGE
The proximal portion gives the Malleus and
Incus, two of the bones of the middle ear.
The distal portion gives rise to the cartilaginous
remnants in the midline of the mandible.
The middle portion is replaced by fibrous tissue,
which persists to form the sphenomandibular
ligament.
17.
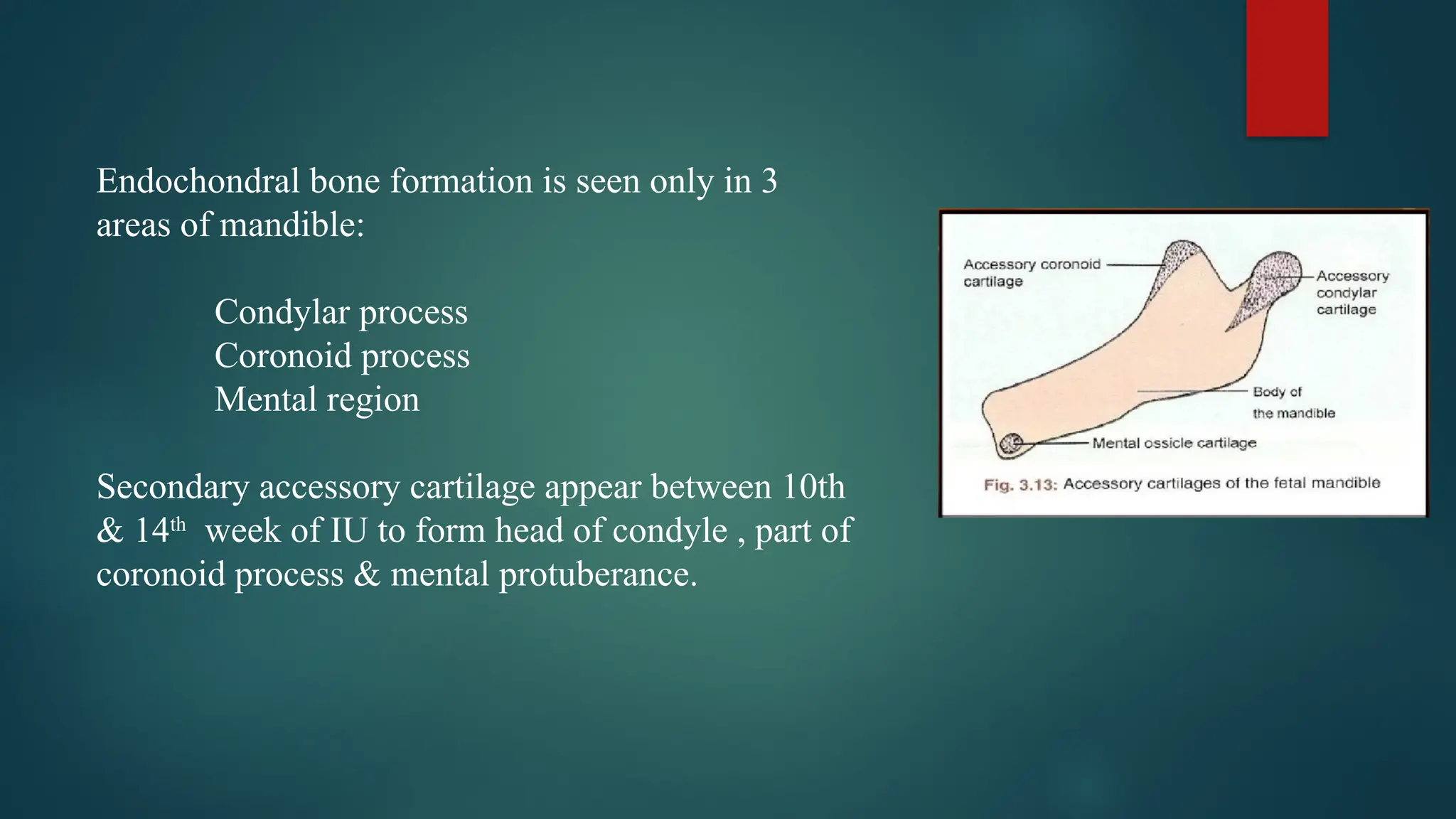
Endochondral bone formationis seen only in 3
areas of mandible:
Condylar process
Coronoid process
Mental region
Secondary accessory cartilage appear between 10th
& 14th
week of IU to form head of condyle , part of
coronoid process & mental protuberance.
18.
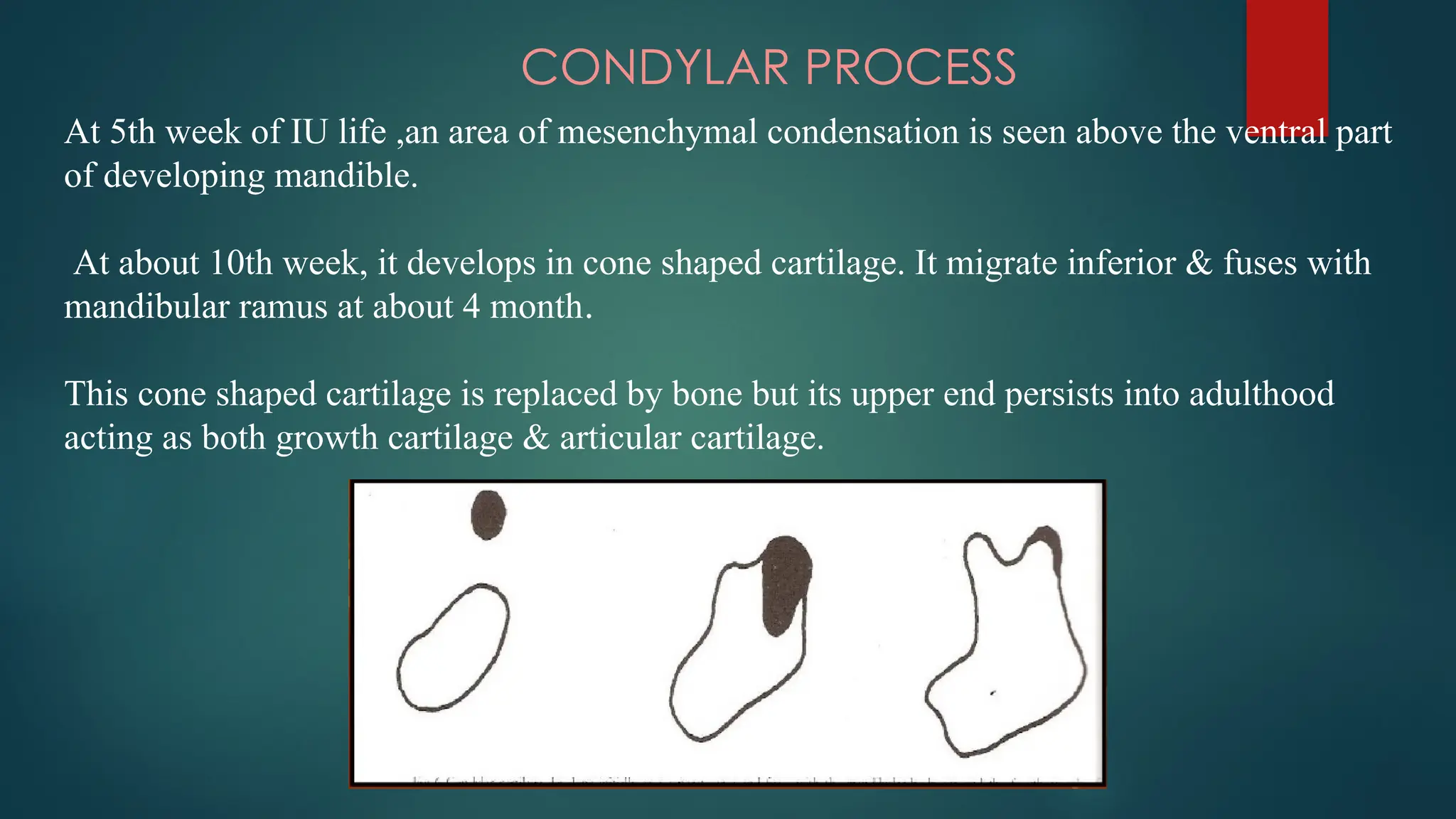
CONDYLAR PROCESS
At 5thweek of IU life ,an area of mesenchymal condensation is seen above the ventral part
of developing mandible.
At about 10th week, it develops in cone shaped cartilage. It migrate inferior & fuses with
mandibular ramus at about 4 month.
This cone shaped cartilage is replaced by bone but its upper end persists into adulthood
acting as both growth cartilage & articular cartilage.
19.
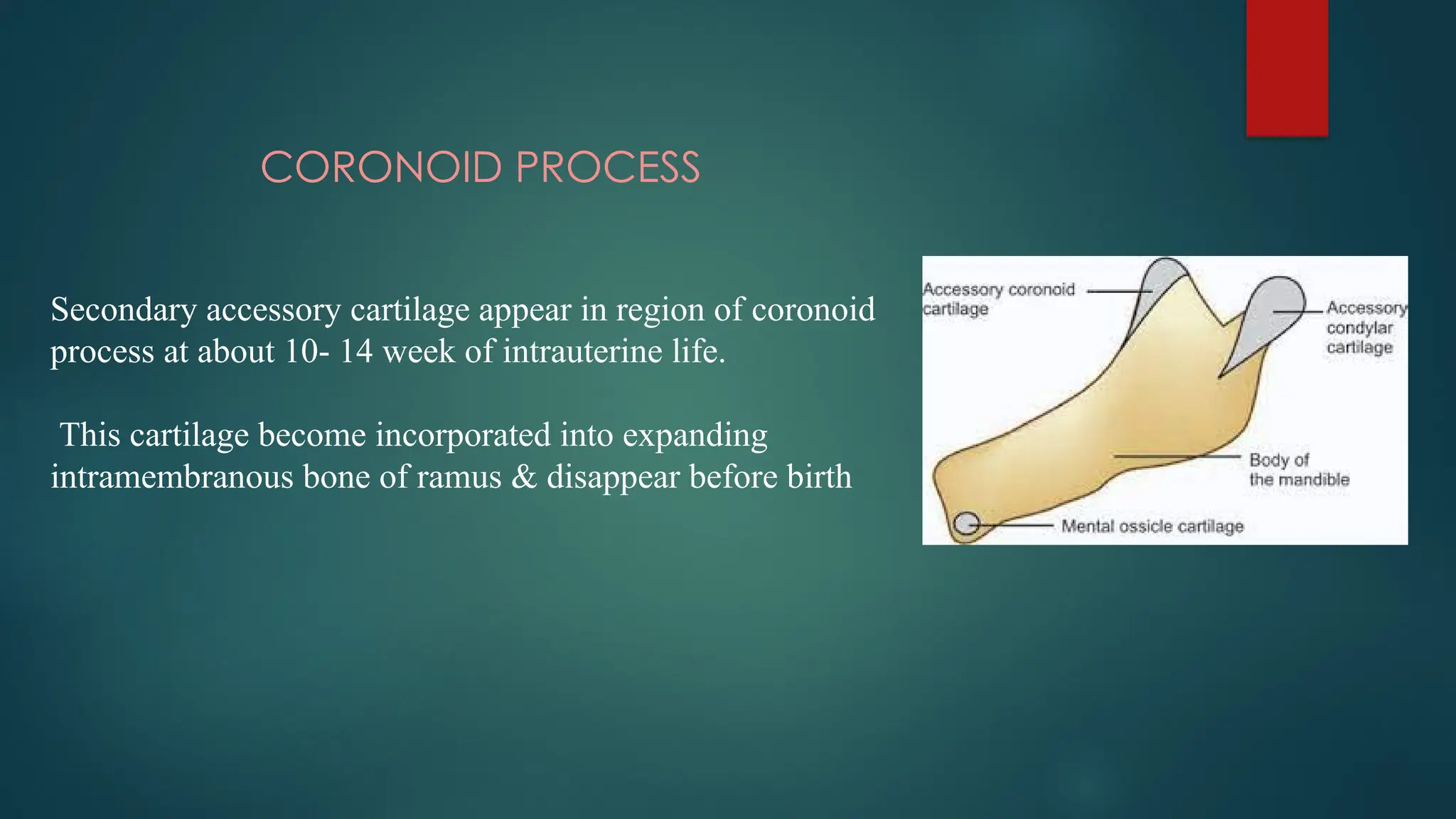
CORONOID PROCESS
Secondary accessorycartilage appear in region of coronoid
process at about 10- 14 week of intrauterine life.
This cartilage become incorporated into expanding
intramembranous bone of ramus & disappear before birth
20.
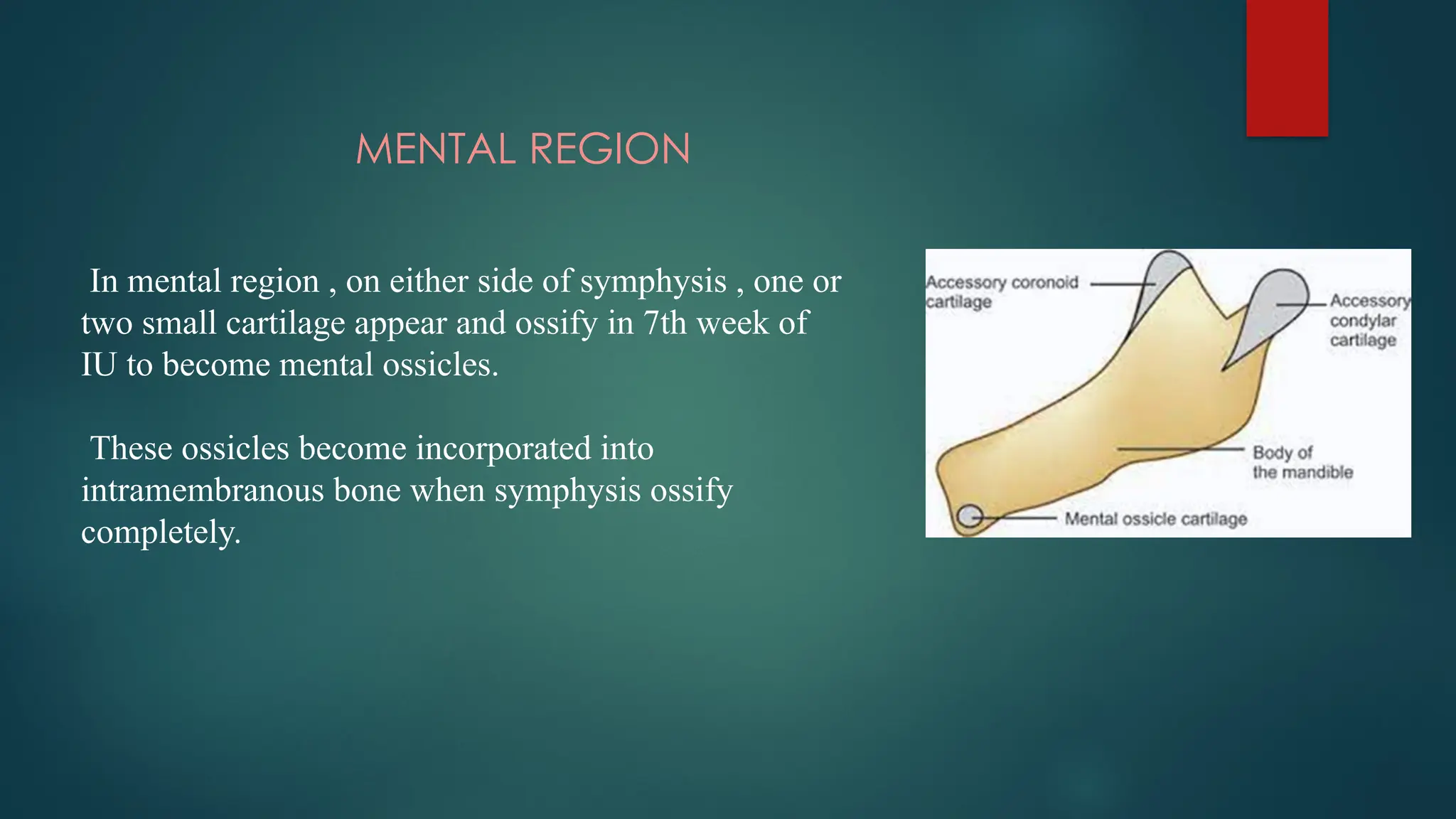
MENTAL REGION
In mentalregion , on either side of symphysis , one or
two small cartilage appear and ossify in 7th week of
IU to become mental ossicles.
These ossicles become incorporated into
intramembranous bone when symphysis ossify
completely.
21.
DEVELOPMENT OF ALVEOLARPROCESS
At the end of the 2nd
month of fetal life the maxilla & mandible
forms a groove that is open towards the surface of the oral cavity.
As the tooth develops, so does the alveolar bone which keeps pace
with the lengthening of roots.
At first , alveolar process forms labial and lingual plates between
which a trench is formed where the tooth organs develop.
22.
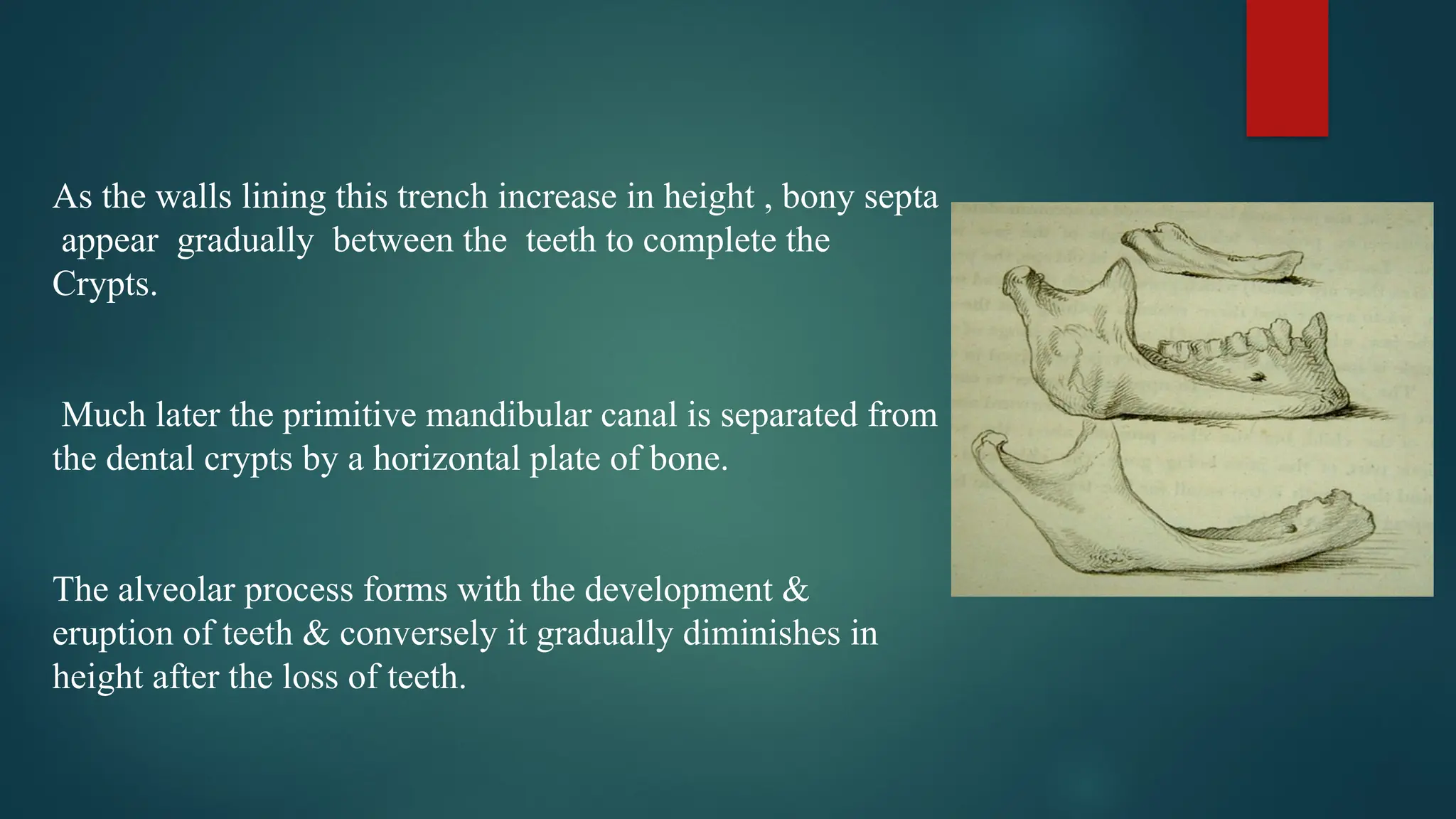
As the wallslining this trench increase in height , bony septa
appear gradually between the teeth to complete the
Crypts.
Much later the primitive mandibular canal is separated from
the dental crypts by a horizontal plate of bone.
The alveolar process forms with the development &
eruption of teeth & conversely it gradually diminishes in
height after the loss of teeth.
23.
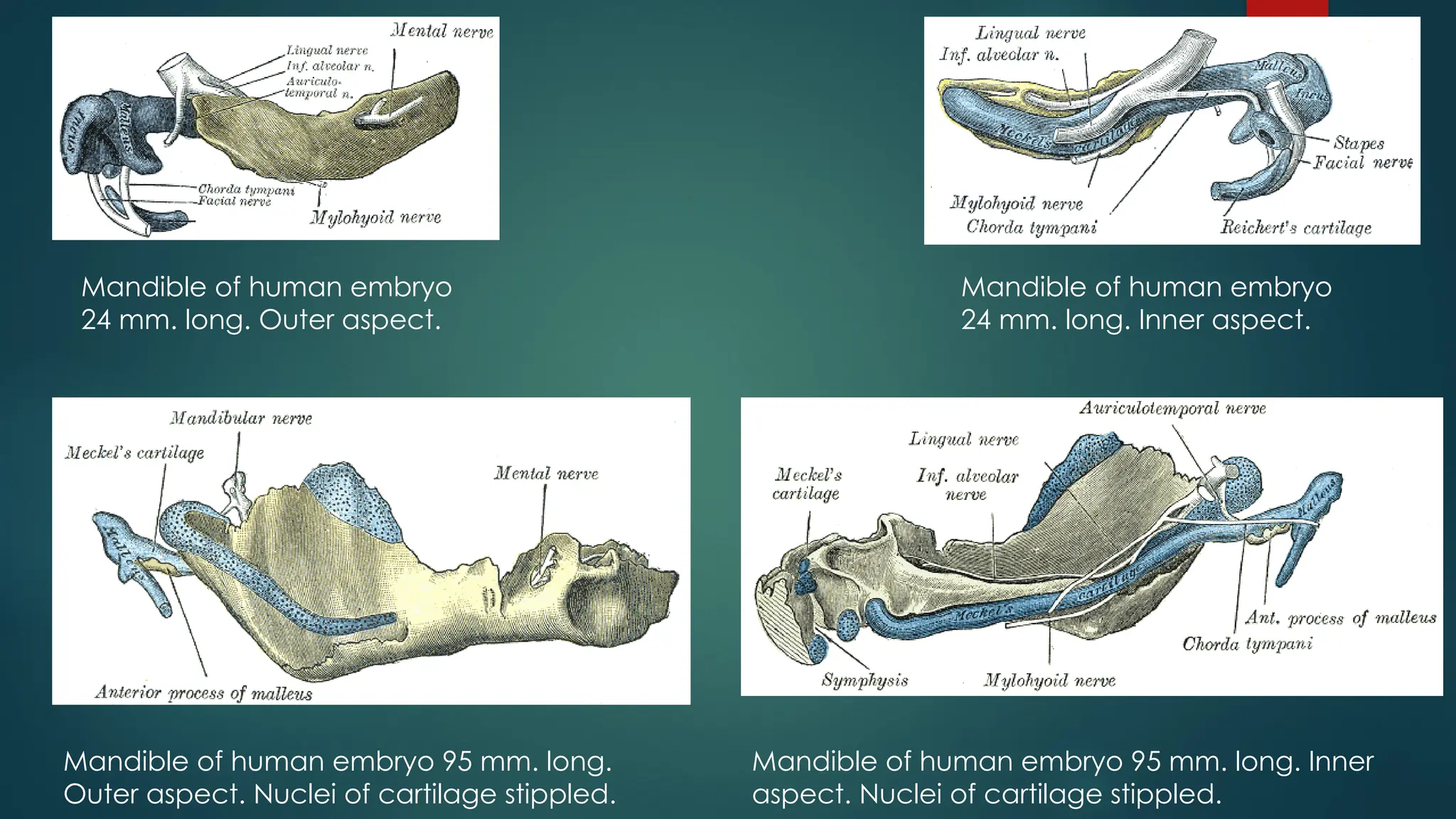
Mandible of humanembryo
24 mm. long. Outer aspect.
Mandible of human embryo
24 mm. long. Inner aspect.
Mandible of human embryo 95 mm. long.
Outer aspect. Nuclei of cartilage stippled.
Mandible of human embryo 95 mm. long. Inner
aspect. Nuclei of cartilage stippled.
24.
SUMMARY OF EVENTS
24 days-formation of mandibular arch.
27 days-appearance of mandibular division of trigeminal
nerve.
36 days-formation of osteogenic membrane.
42 days-first ossification center between incisive and mental branch
of inferior alveolar nerve.
55 days – beginning of coronoid and condyle.
Before end of 2nd
month – tooth germs distinguished.
Fetus at mid term – mandible consists of body and alveolar process.
4 ½ months I.U.L. – adult form recognized.
25.
POST NATAL GROWTHOF MANDIBLE
Of the facial bones, mandible undergoes the largest amount of growth post-natally and
also exhibits largest variability in morphology.
While in the adults it appears as a single bone, it is developmentally and functionally
divisible into several skeletal sub-units like:
Ramus
Body of mandible
Angle of mandible
Lingual tuberosity
Alveolar process
Condyle
Coronoid process
Mental protuberance
26.
RAMUS
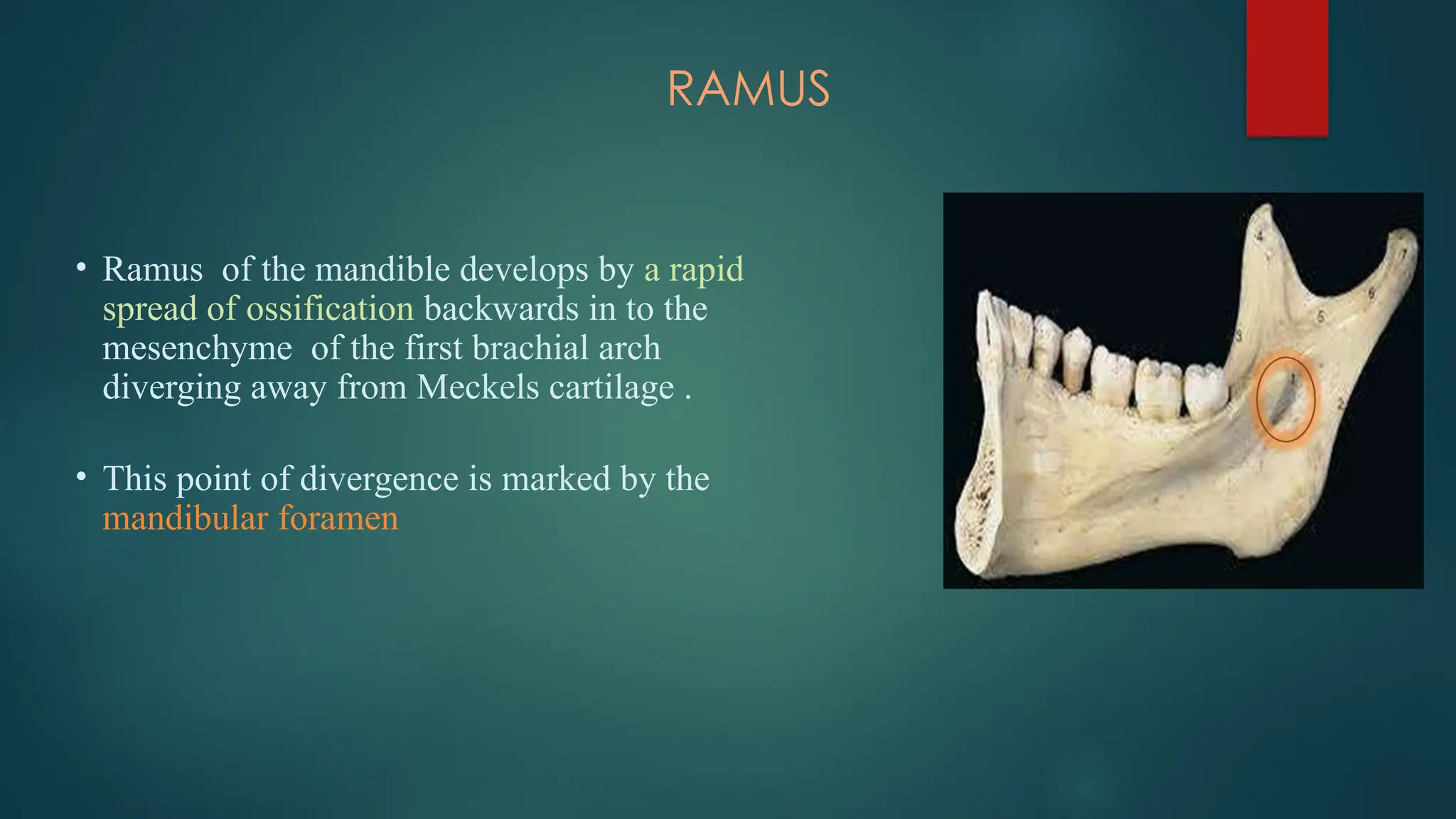
• Ramus ofthe mandible develops by a rapid
spread of ossification backwards in to the
mesenchyme of the first brachial arch
diverging away from Meckels cartilage .
• This point of divergence is marked by the
mandibular foramen
27.
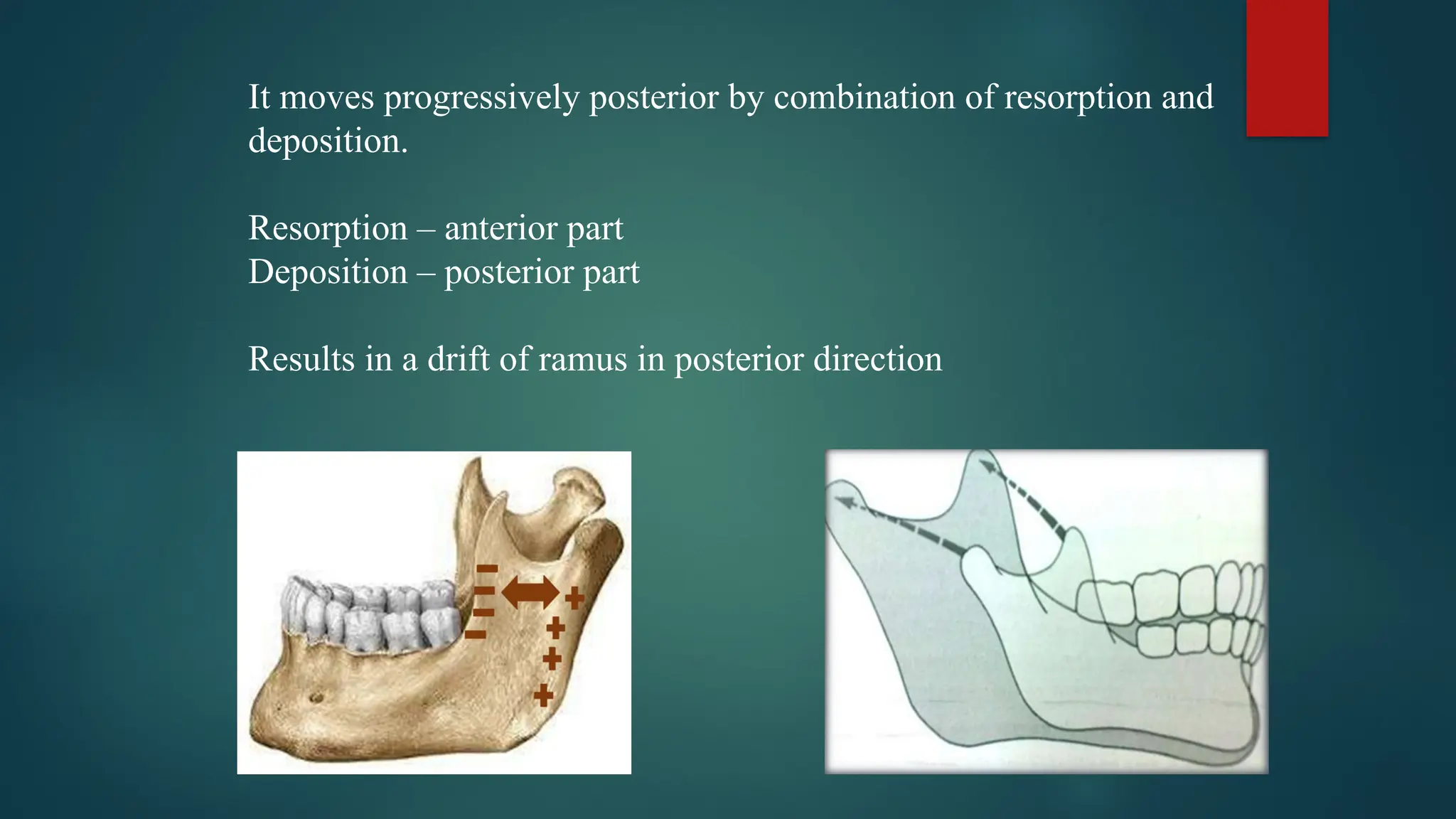
It moves progressivelyposterior by combination of resorption and
deposition.
Resorption – anterior part
Deposition – posterior part
Results in a drift of ramus in posterior direction
28.
ANGLE OF MANDIBLE
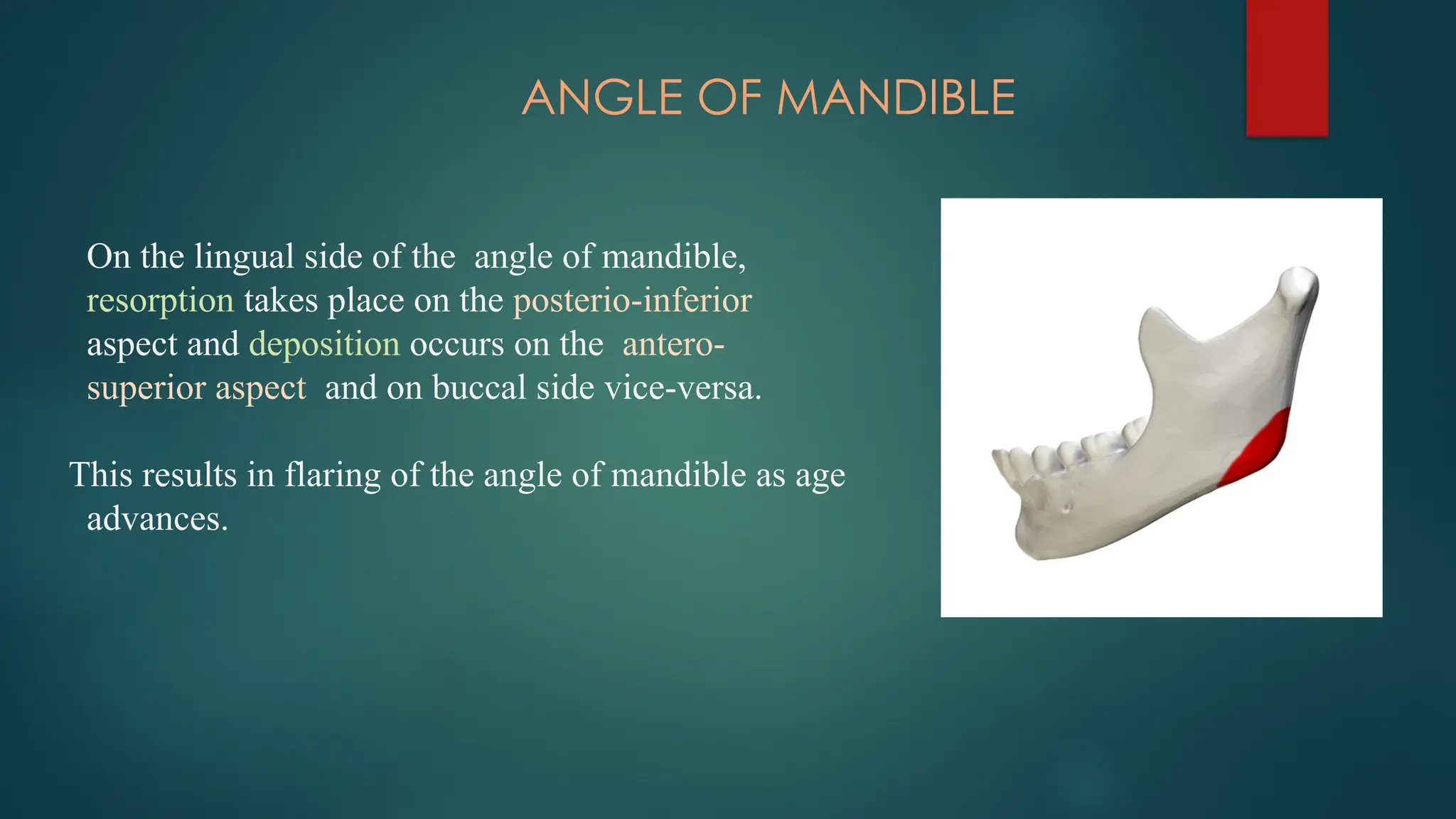
Onthe lingual side of the angle of mandible,
resorption takes place on the posterio-inferior
aspect and deposition occurs on the antero-
superior aspect and on buccal side vice-versa.
This results in flaring of the angle of mandible as age
advances.
29.
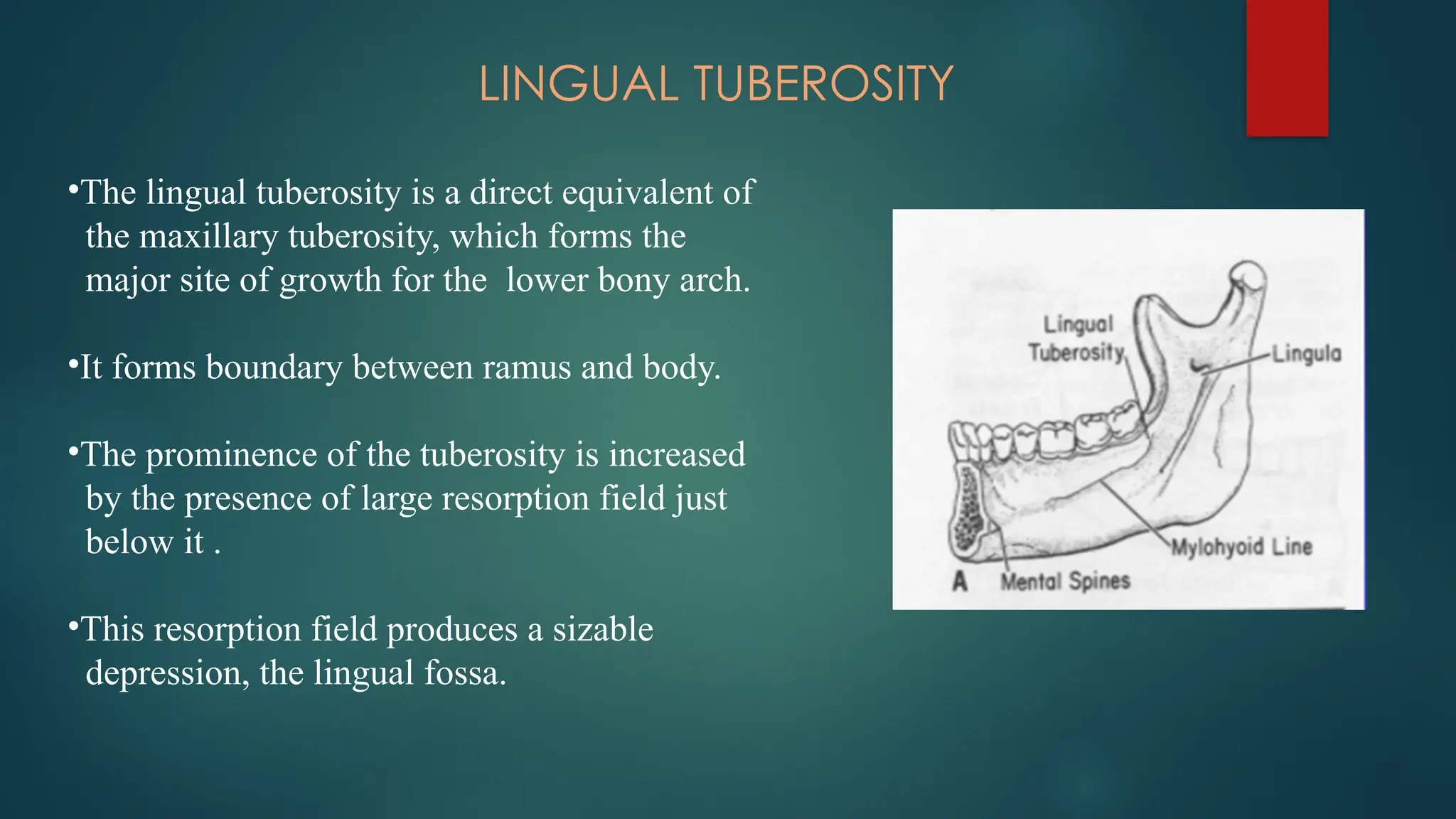
LINGUAL TUBEROSITY
•The lingualtuberosity is a direct equivalent of
the maxillary tuberosity, which forms the
major site of growth for the lower bony arch.
•It forms boundary between ramus and body.
•The prominence of the tuberosity is increased
by the presence of large resorption field just
below it .
•This resorption field produces a sizable
depression, the lingual fossa.
30.
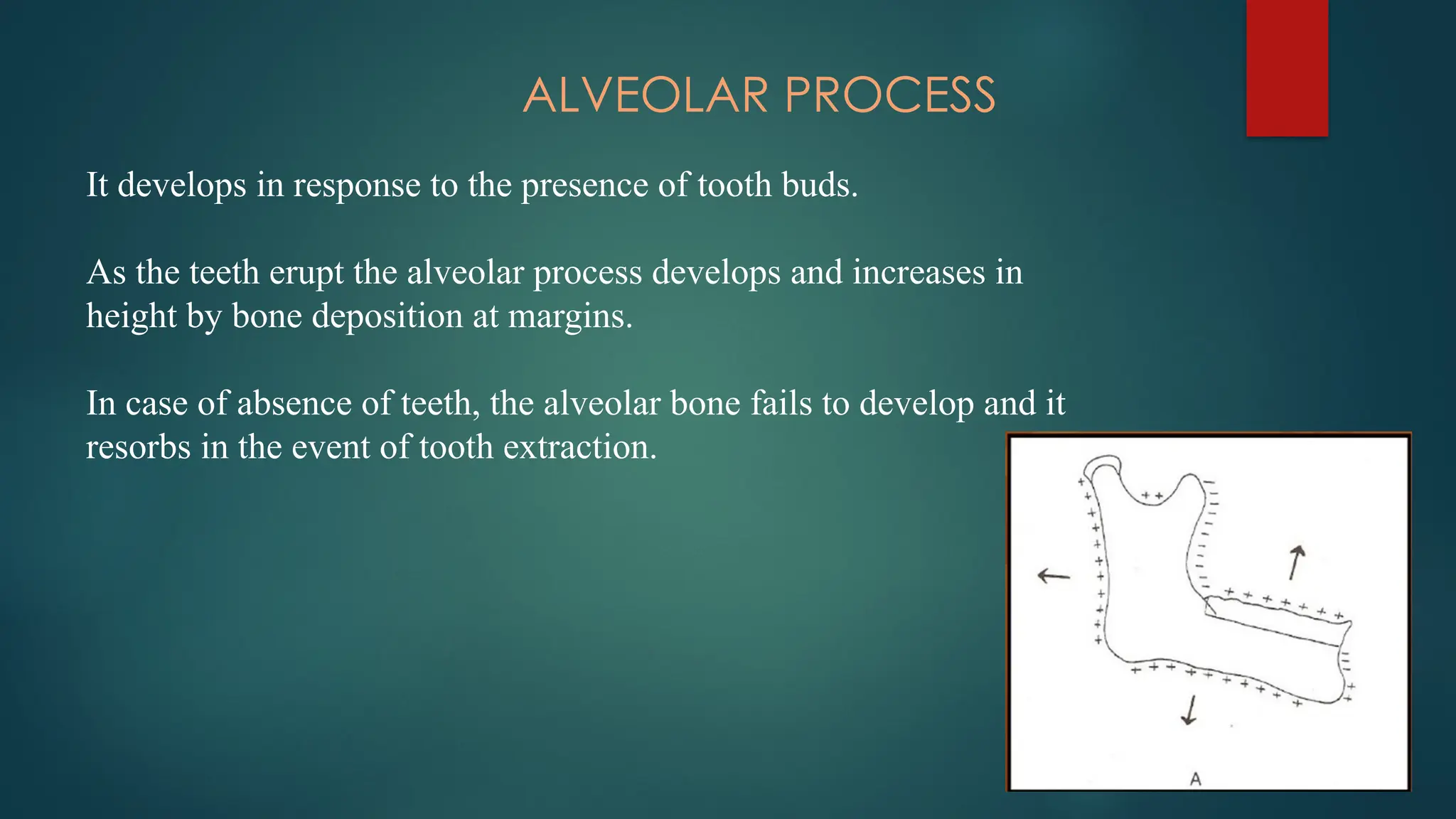
ALVEOLAR PROCESS
It developsin response to the presence of tooth buds.
As the teeth erupt the alveolar process develops and increases in
height by bone deposition at margins.
In case of absence of teeth, the alveolar bone fails to develop and it
resorbs in the event of tooth extraction.
31.
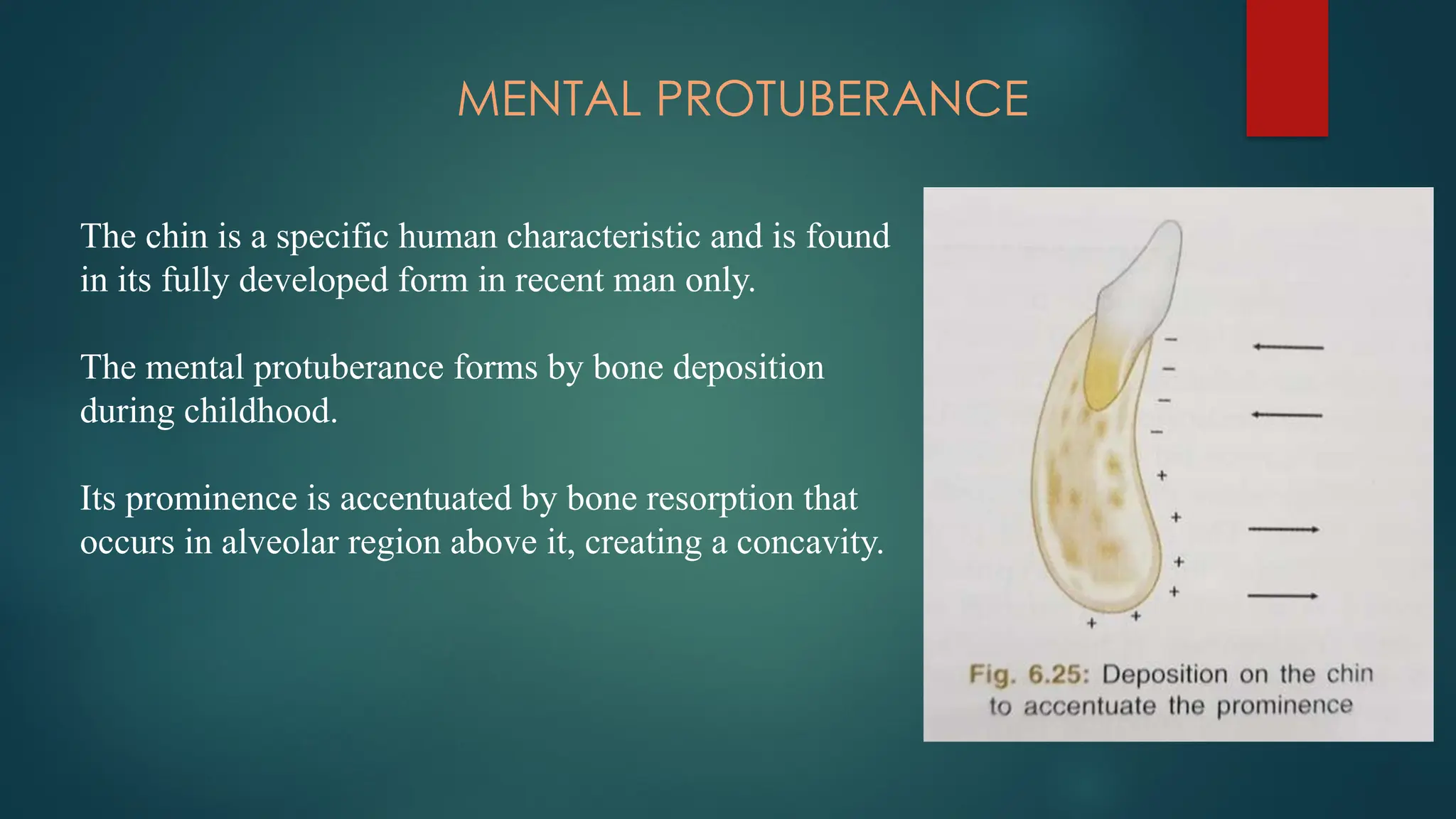
MENTAL PROTUBERANCE
The chinis a specific human characteristic and is found
in its fully developed form in recent man only.
The mental protuberance forms by bone deposition
during childhood.
Its prominence is accentuated by bone resorption that
occurs in alveolar region above it, creating a concavity.
32.
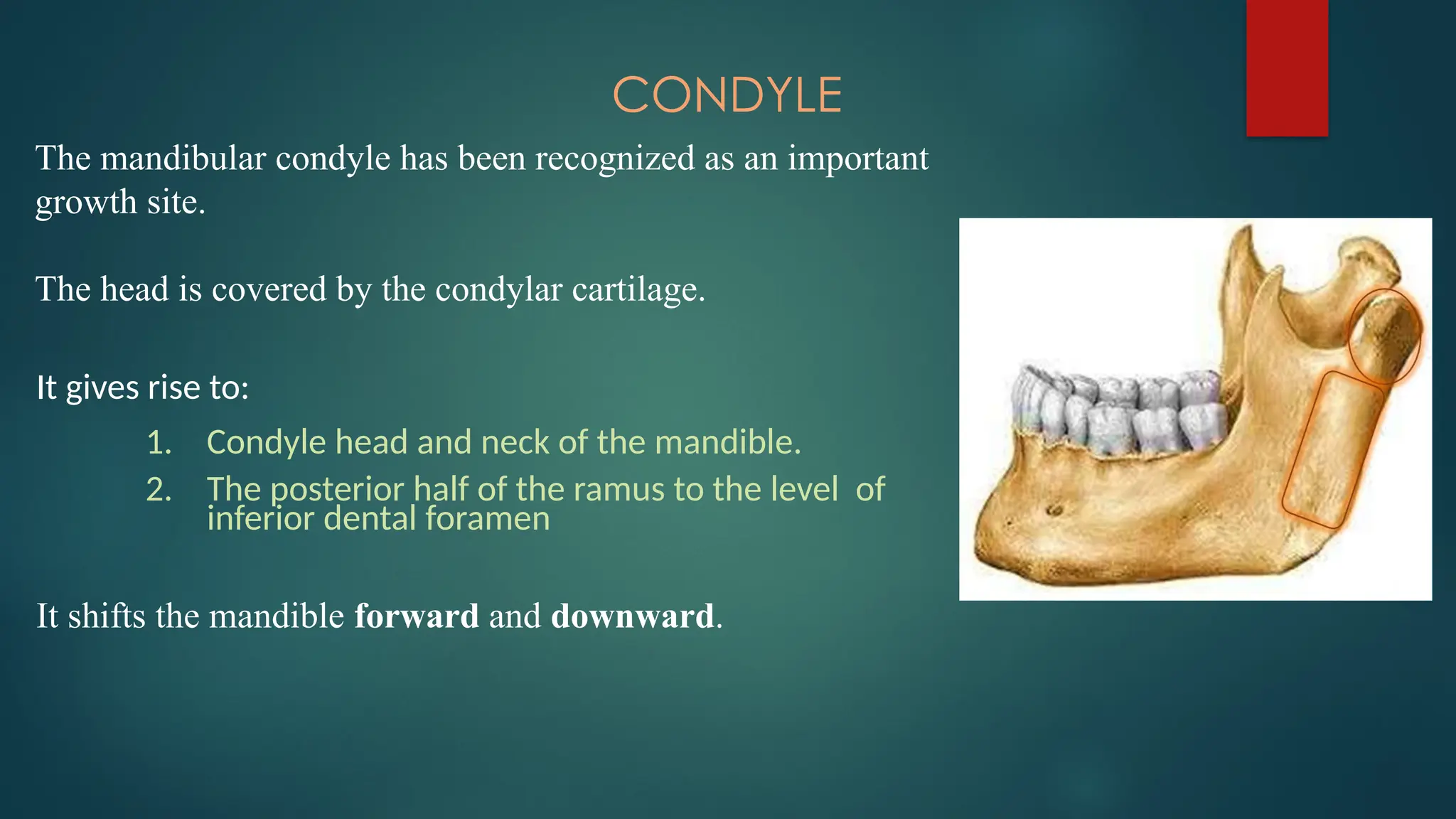
CONDYLE
The mandibular condylehas been recognized as an important
growth site.
The head is covered by the condylar cartilage.
It gives rise to:
1. Condyle head and neck of the mandible.
2. The posterior half of the ramus to the level of
inferior dental foramen
It shifts the mandible forward and downward.
33.
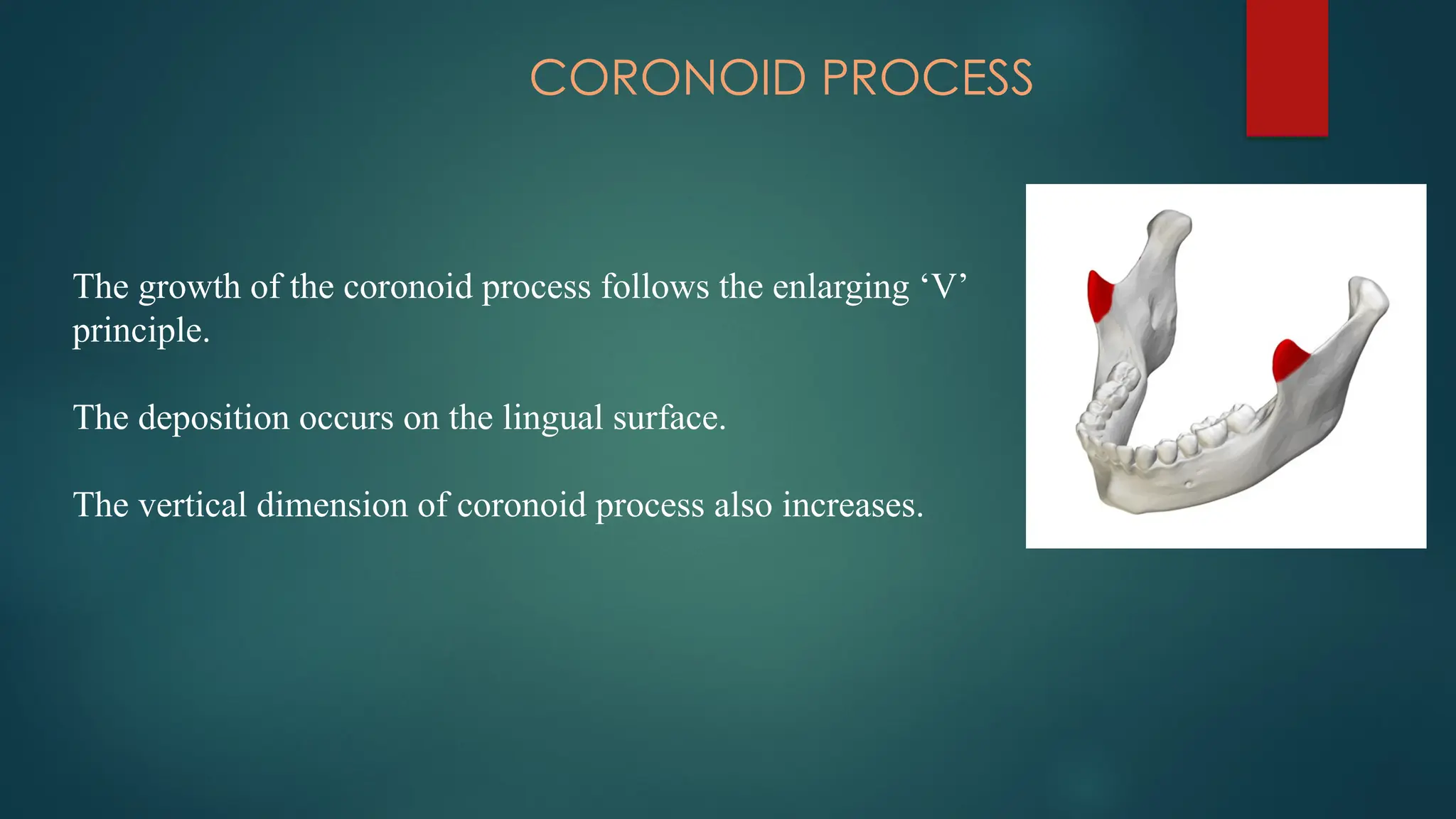
CORONOID PROCESS
The growthof the coronoid process follows the enlarging ‘V’
principle.
The deposition occurs on the lingual surface.
The vertical dimension of coronoid process also increases.
34.
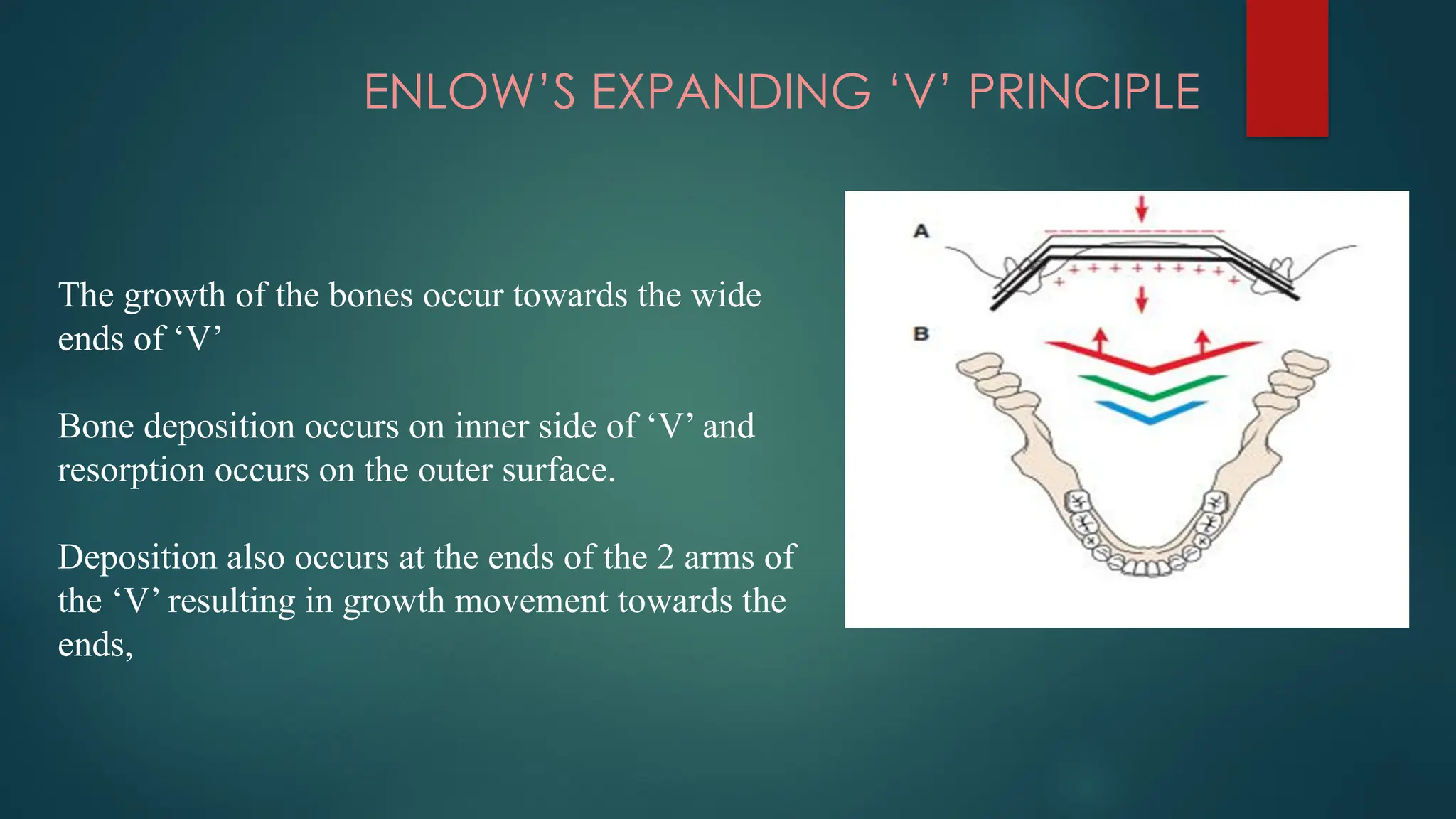
ENLOW’S EXPANDING ‘V’PRINCIPLE
The growth of the bones occur towards the wide
ends of ‘V’
Bone deposition occurs on inner side of ‘V’ and
resorption occurs on the outer surface.
Deposition also occurs at the ends of the 2 arms of
the ‘V’ resulting in growth movement towards the
ends,
35.
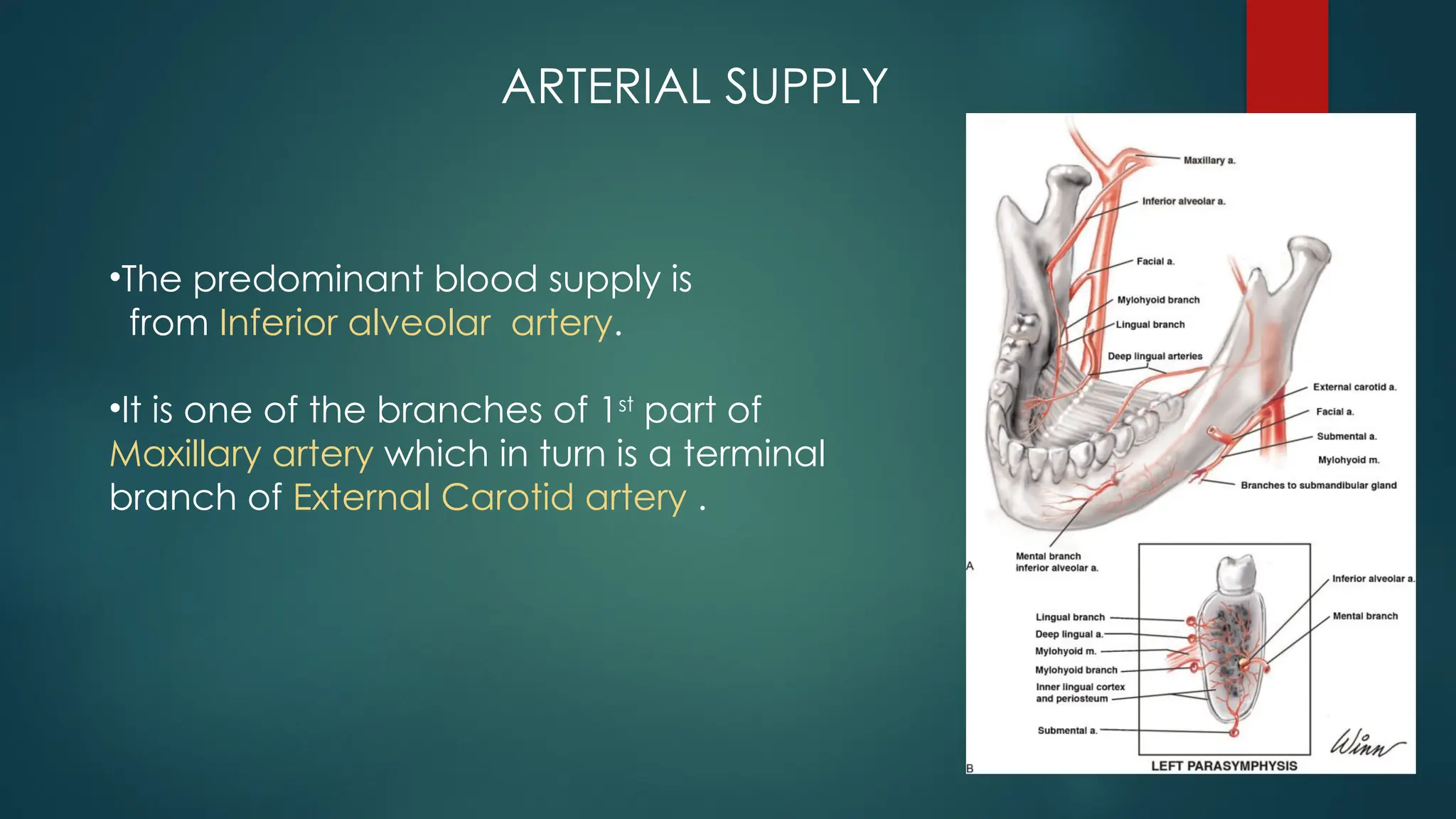
ARTERIAL SUPPLY
•The predominantblood supply is
from Inferior alveolar artery.
•It is one of the branches of 1st
part of
Maxillary artery which in turn is a terminal
branch of External Carotid artery .
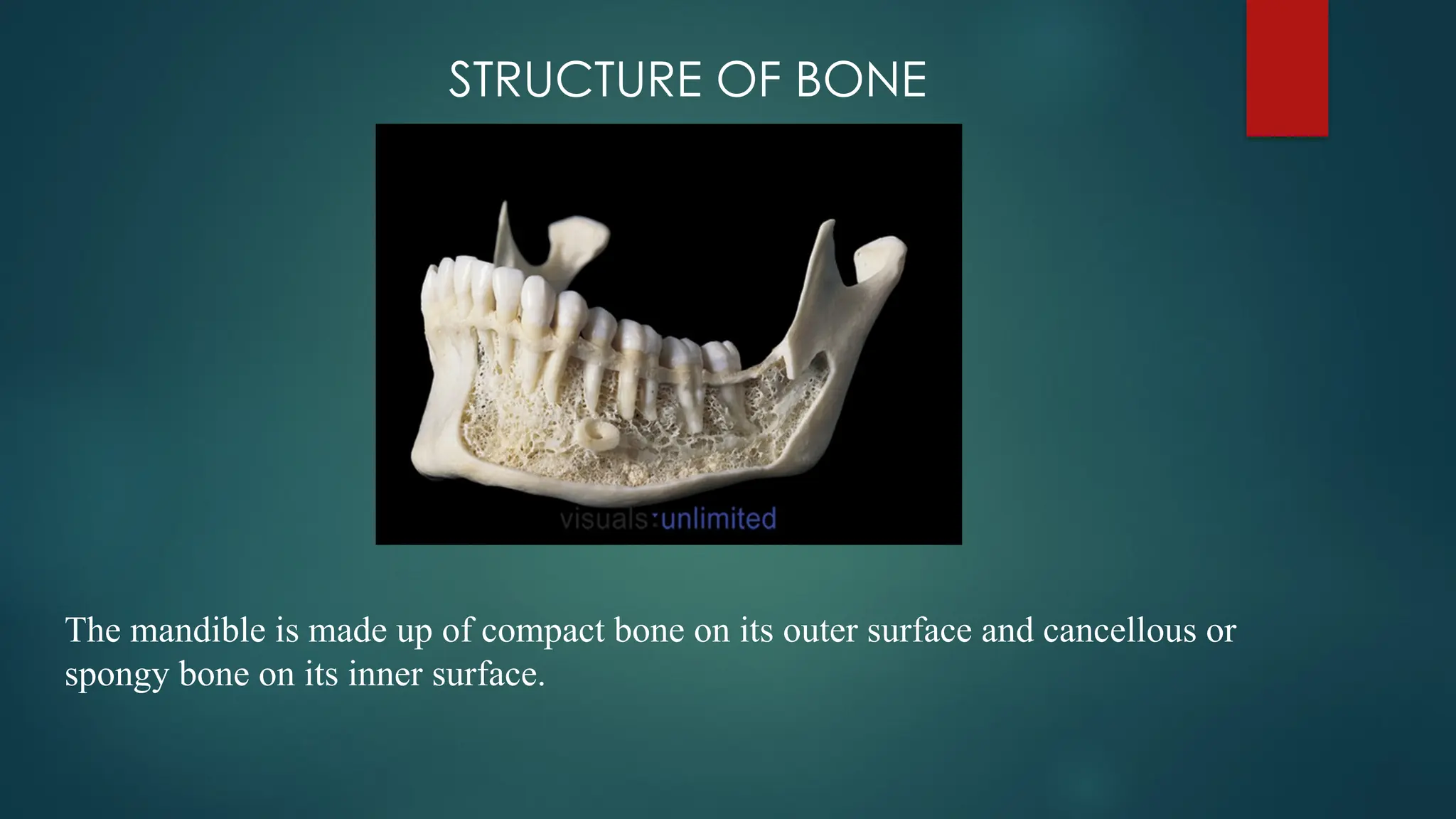
STRUCTURE OF BONE
Themandible is made up of compact bone on its outer surface and cancellous or
spongy bone on its inner surface.
41.
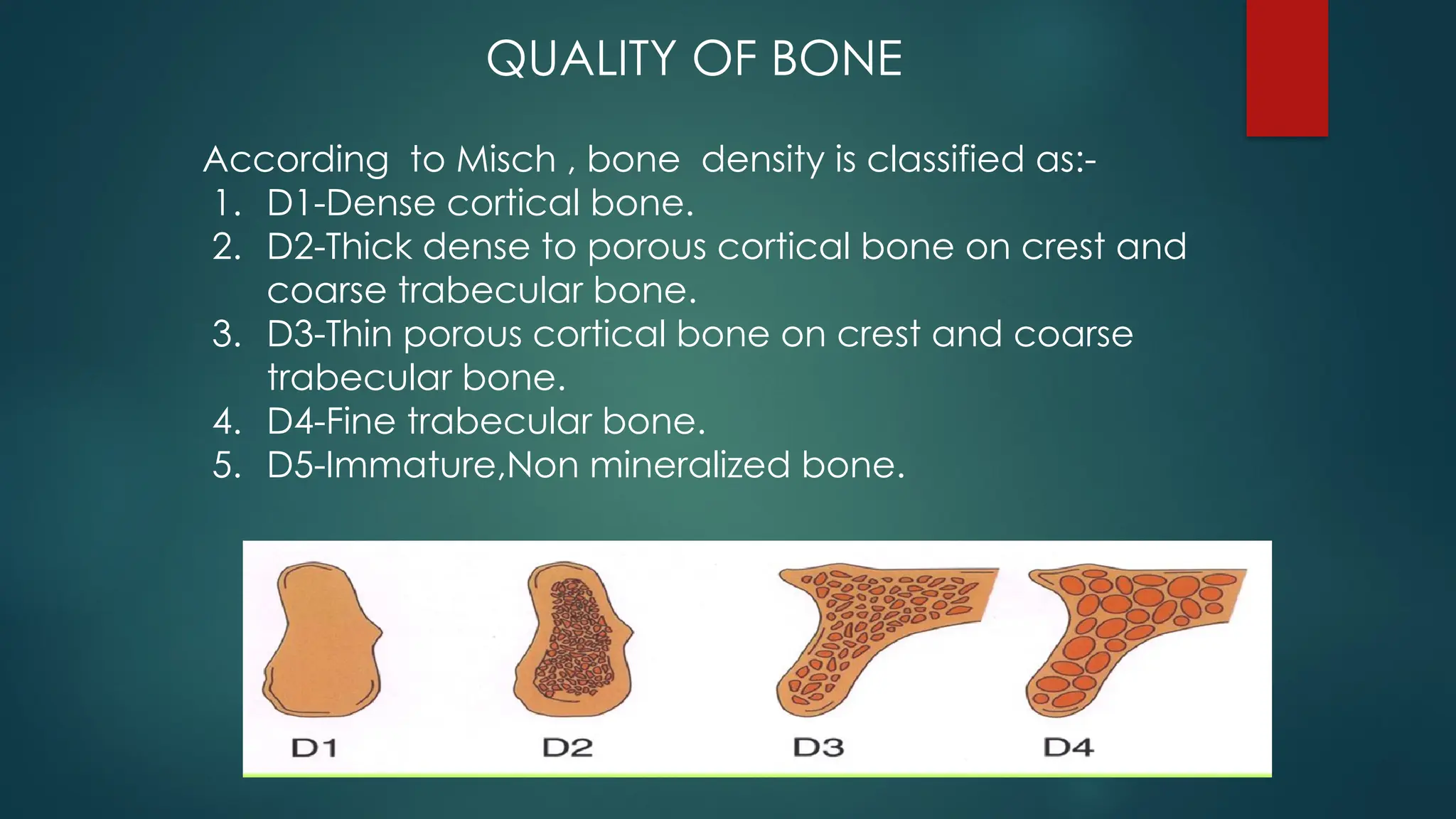
According to Misch, bone density is classified as:-
1. D1-Dense cortical bone.
2. D2-Thick dense to porous cortical bone on crest and
coarse trabecular bone.
3. D3-Thin porous cortical bone on crest and coarse
trabecular bone.
4. D4-Fine trabecular bone.
5. D5-Immature,Non mineralized bone.
QUALITY OF BONE
42.
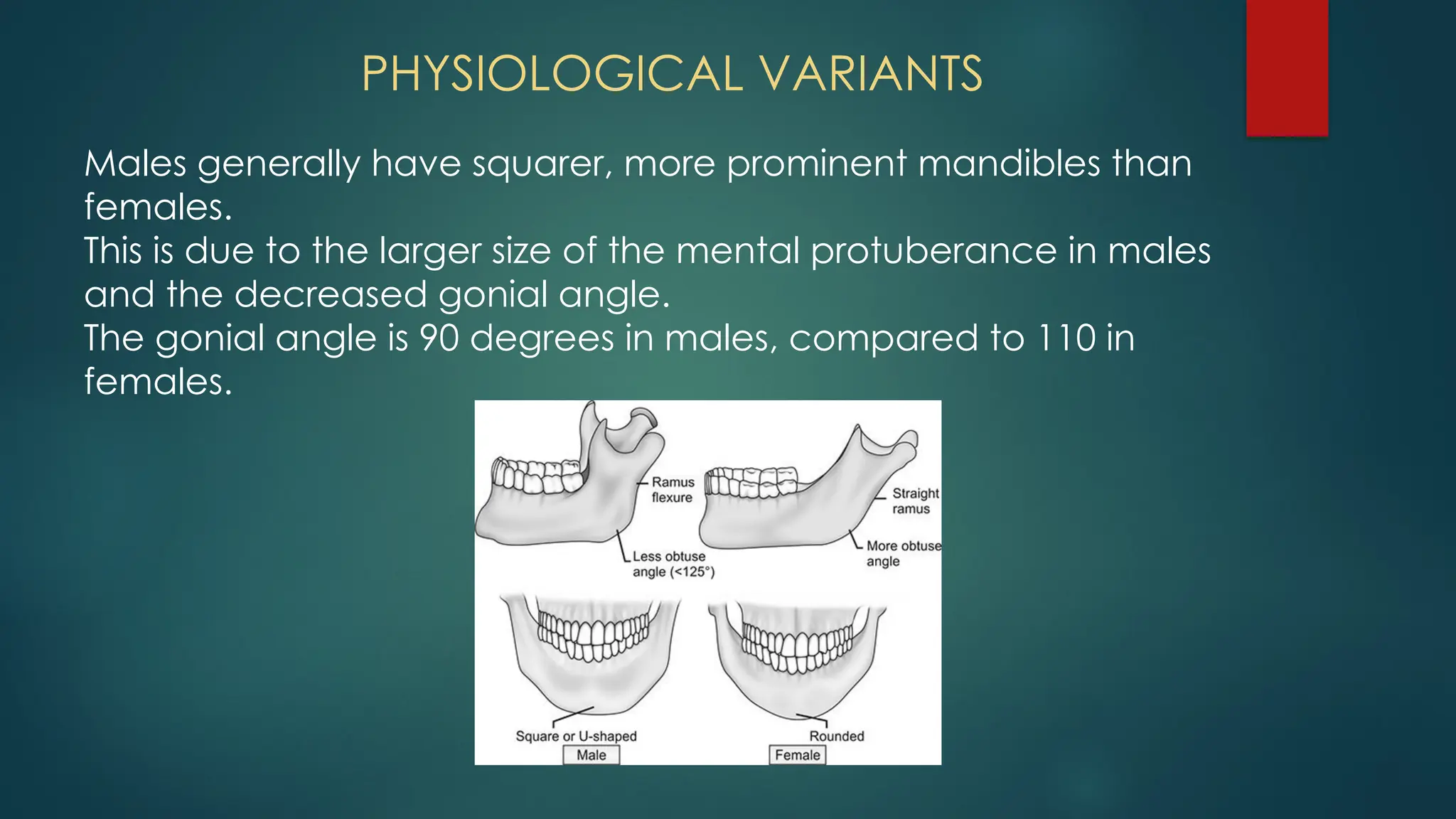
PHYSIOLOGICAL VARIANTS
Males generallyhave squarer, more prominent mandibles than
females.
This is due to the larger size of the mental protuberance in males
and the decreased gonial angle.
The gonial angle is 90 degrees in males, compared to 110 in
females.
43.
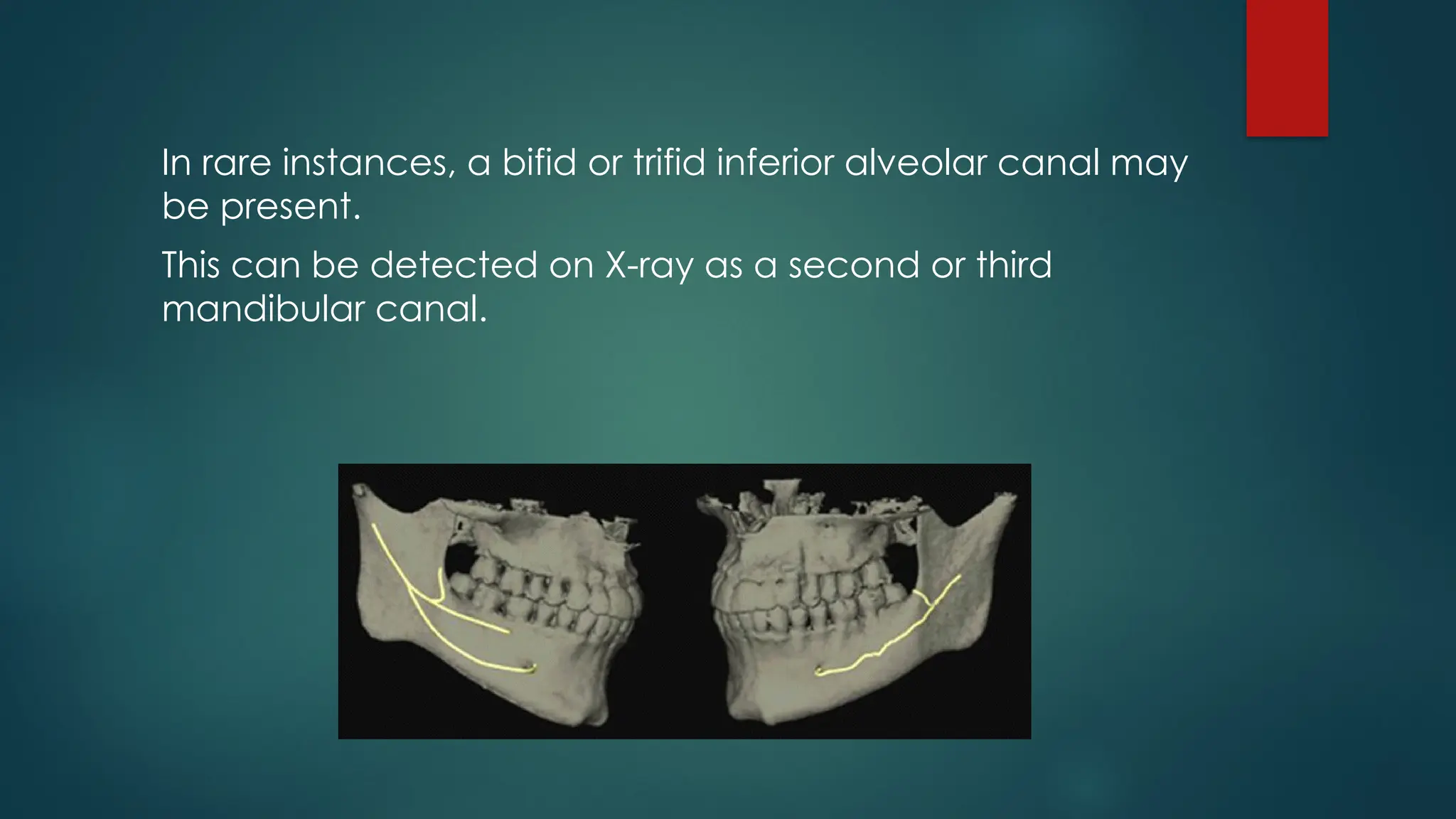
In rare instances,a bifid or trifid inferior alveolar canal may
be present.
This can be detected on X-ray as a second or third
mandibular canal.
44.
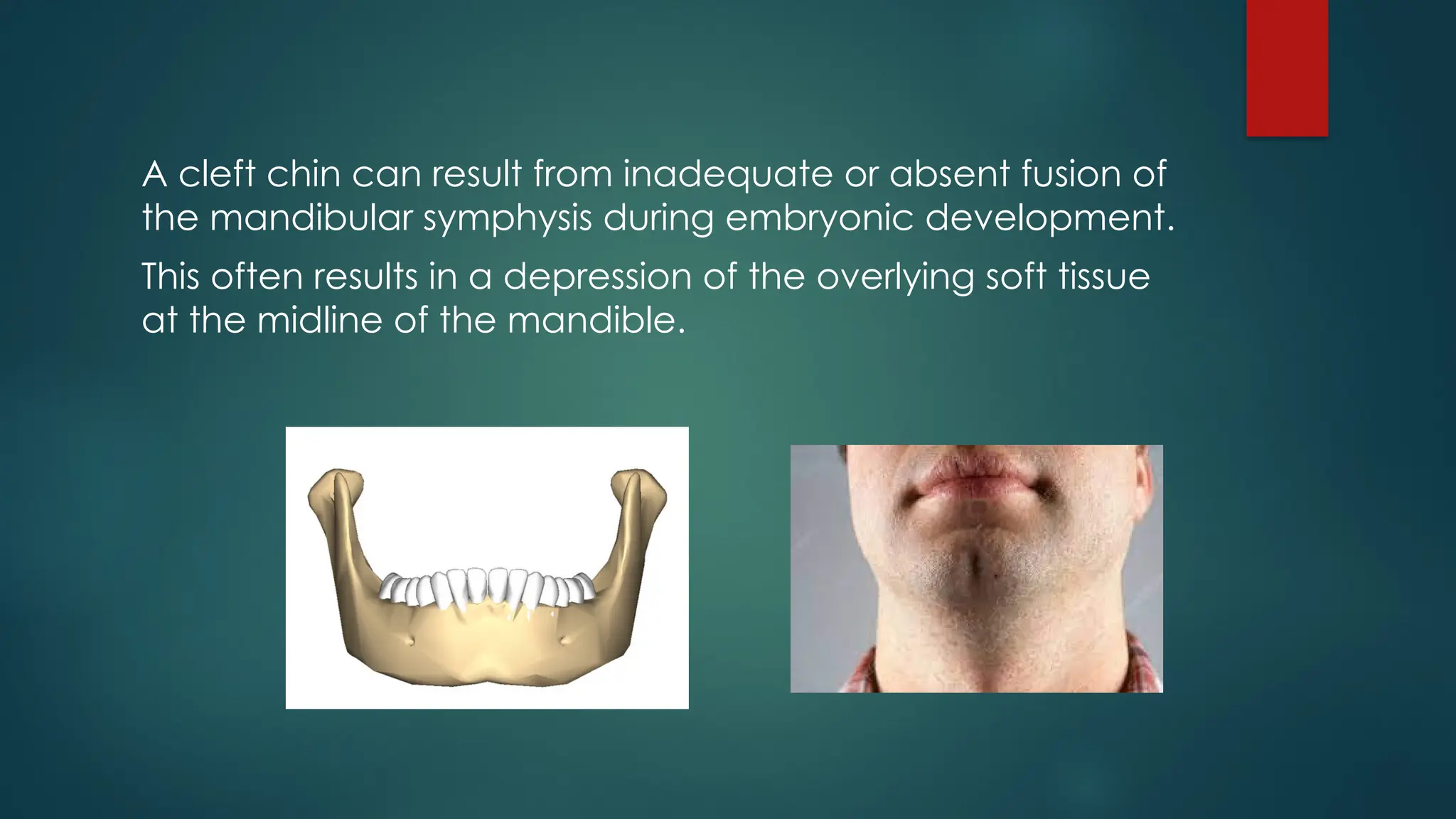
A cleft chincan result from inadequate or absent fusion of
the mandibular symphysis during embryonic development.
This often results in a depression of the overlying soft tissue
at the midline of the mandible.
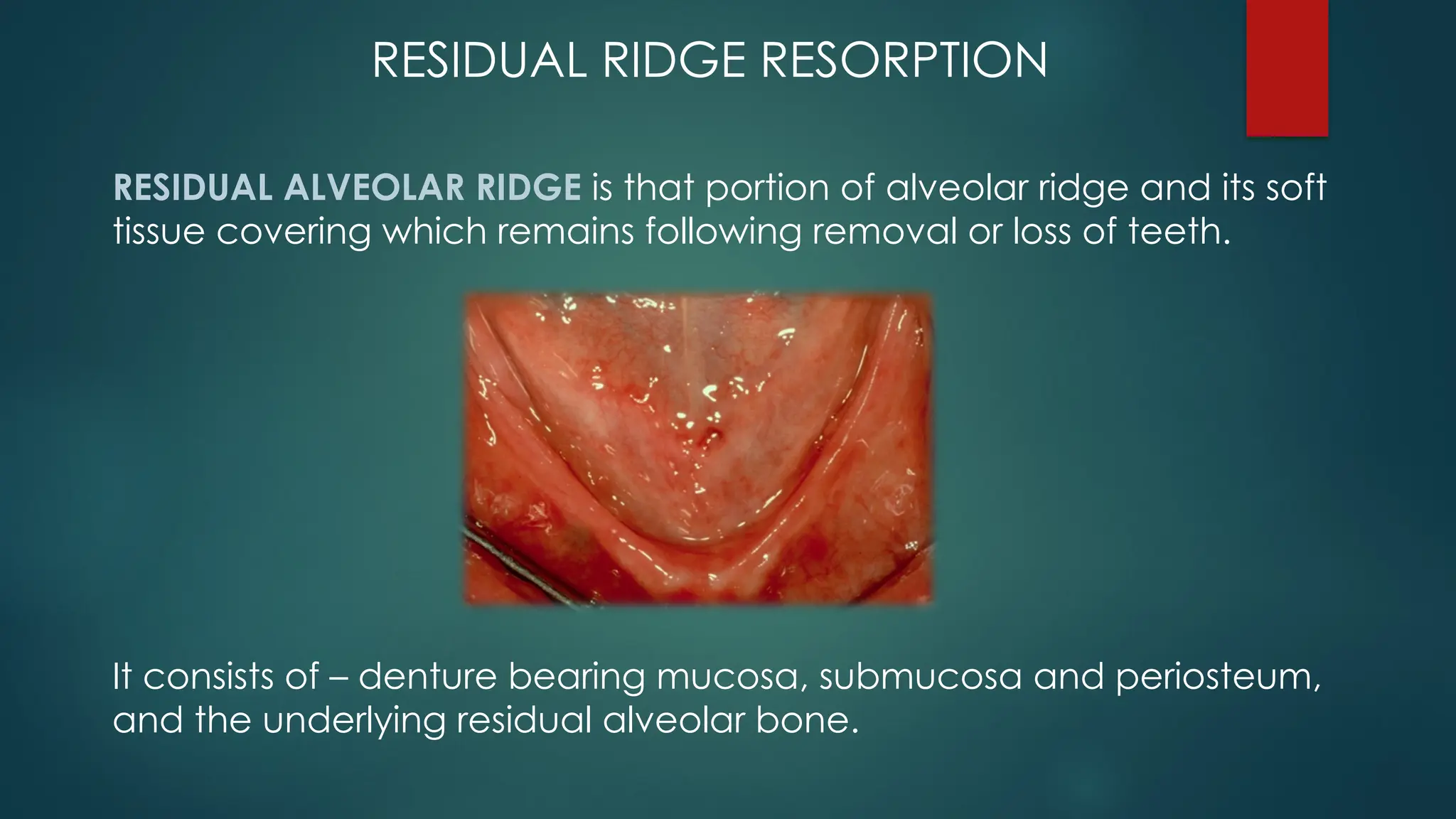
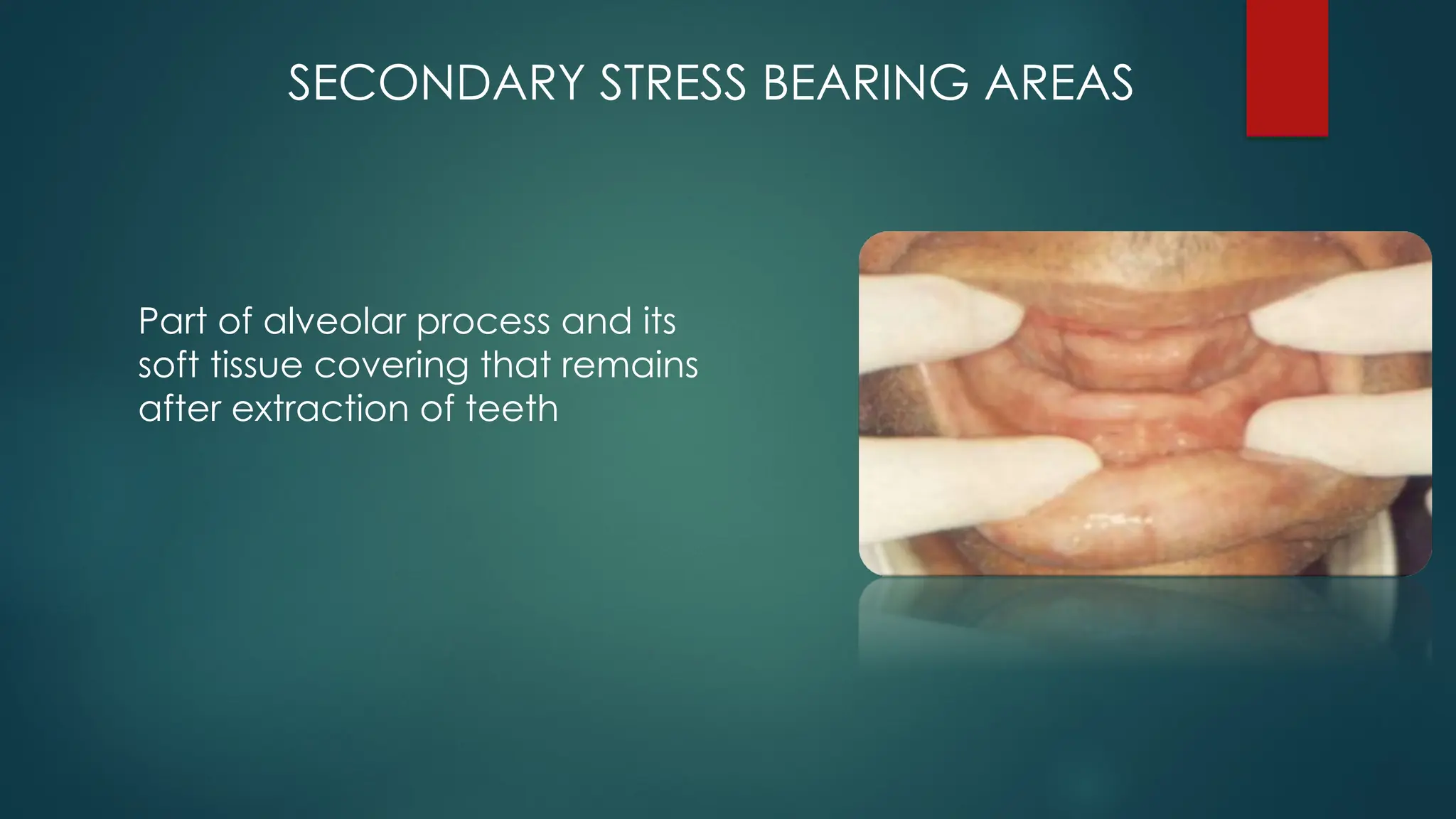
RESIDUAL RIDGE RESORPTION
RESIDUALALVEOLAR RIDGE is that portion of alveolar ridge and its soft
tissue covering which remains following removal or loss of teeth.
It consists of – denture bearing mucosa, submucosa and periosteum,
and the underlying residual alveolar bone.
48.
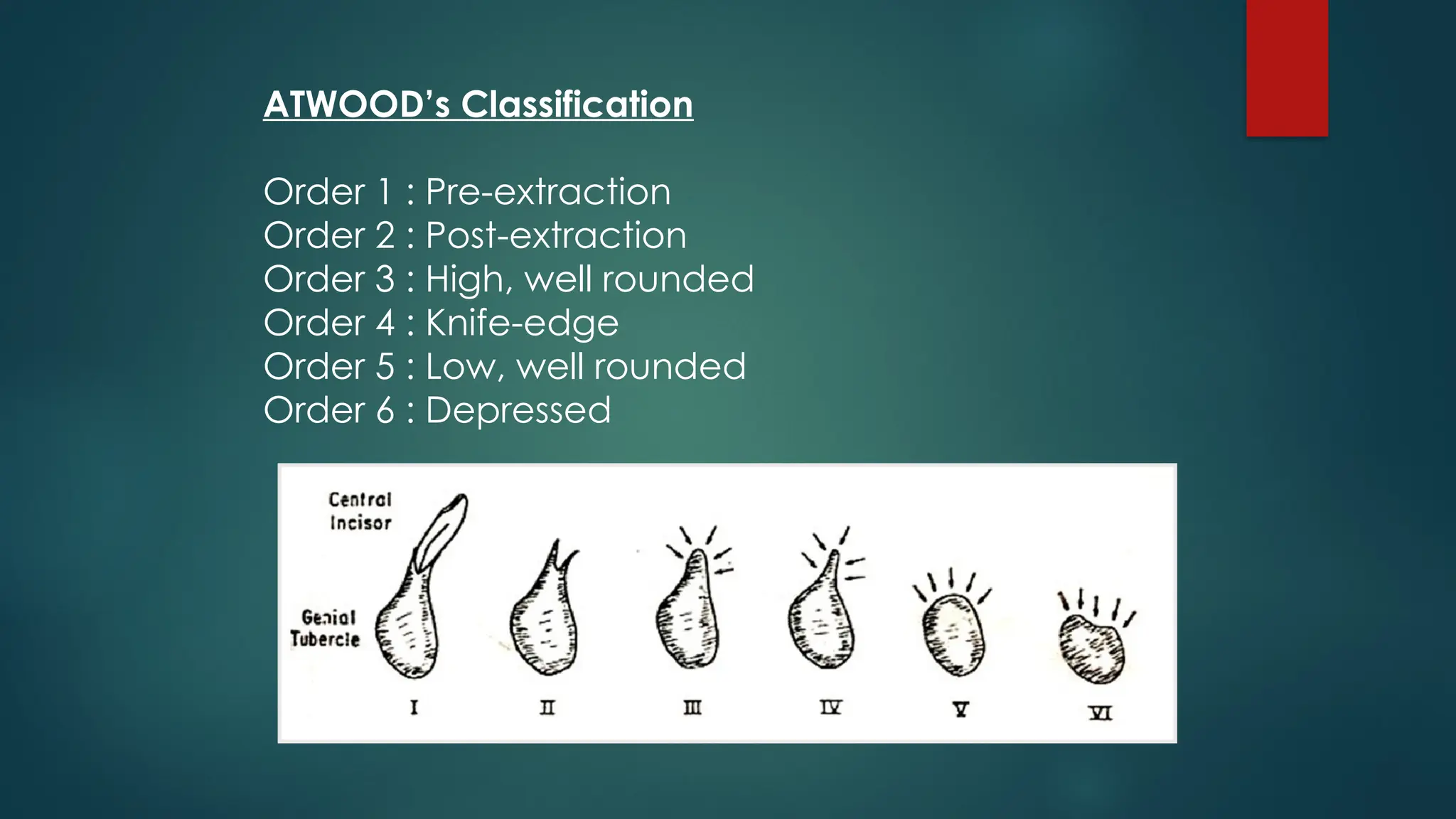
ATWOOD’s Classification
Order 1: Pre-extraction
Order 2 : Post-extraction
Order 3 : High, well rounded
Order 4 : Knife-edge
Order 5 : Low, well rounded
Order 6 : Depressed
49.
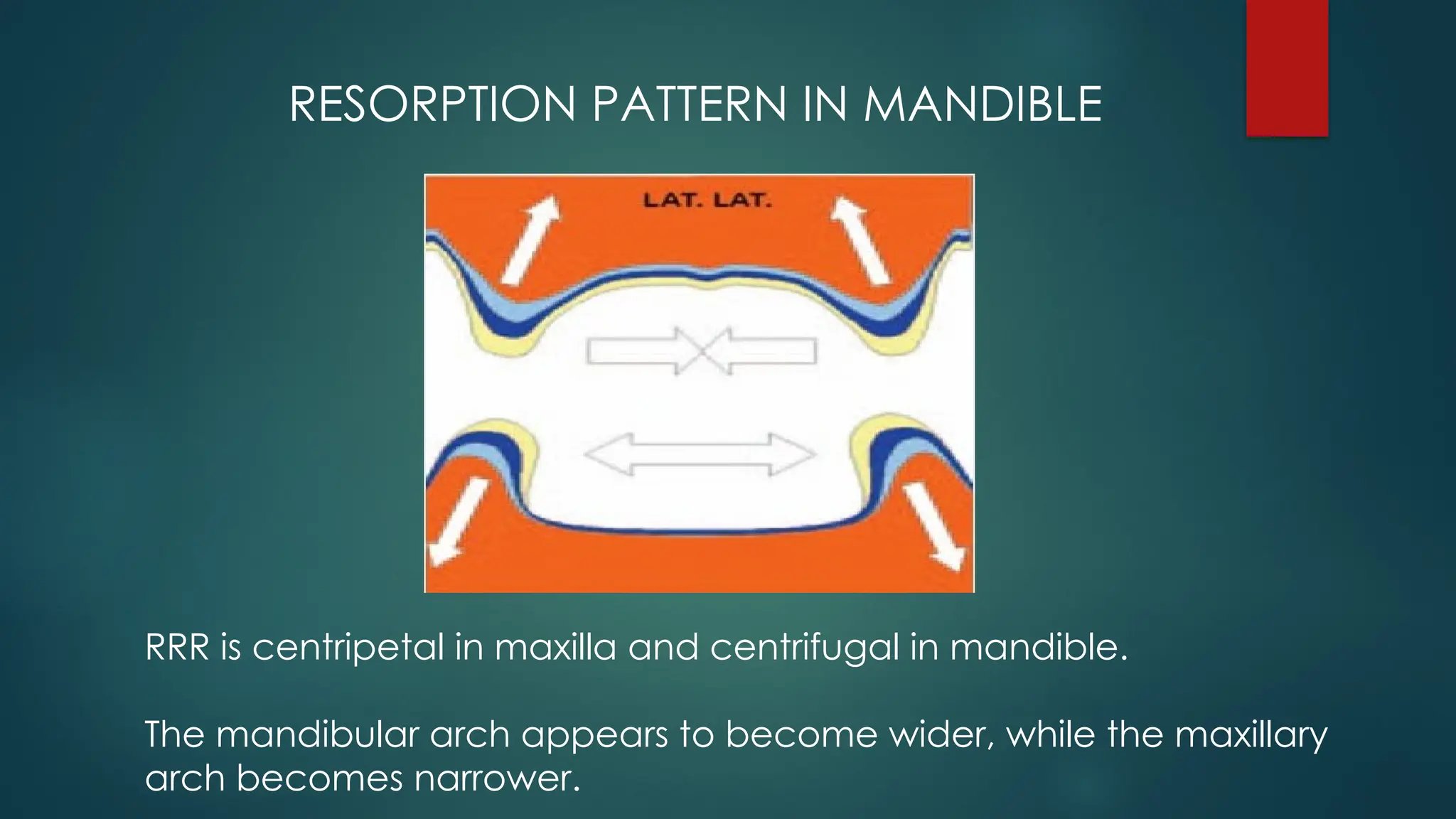
RESORPTION PATTERN INMANDIBLE
RRR is centripetal in maxilla and centrifugal in mandible.
The mandibular arch appears to become wider, while the maxillary
arch becomes narrower.
DEVELOPMENTAL ANAMOLIES OFMANDIBLE:
1. AGNATHIA
2. MICROGNATHIA
3. ACQUIRED MICROGNATHIA
4. MACROGNATHIA - often associated with :
PAGETS DISEASE OF BONE
ACROMEGALY
LEONTIASIS OSSEA
5. FACIAL HEMIHYPERTROPHY
6. MANDIBULAR DYSOSTOSIS
7 .CHERUBISM
8. EXOSTOSES
9. TORUS MANDIBULARIS
57.
CONCLUSION
•Knowledge of themandibular anatomy is necessary
for making impression, recording jaw relations,
adjusting dentures for better outcome.
58.
REFERENCES
B.D.chaurasia Text bookof anatomy vol 3 HEAD AND NECK.
Zarb , bolender, carlson – BOUCHER’S prosthodontic treatment for edentulous
patients,12th
edition
Inderbir singh ,Human anatomy – 7th
edition.
S.I. Bhalajhi, Orthodontics- arts and sciences.
A K Datta ,Human anatomy head and neck .
Nafis Ahmed Faruqi. Human osteology-[clinical orientation]
YI – Pingliu ; Peter – mandibular development , remodelling and age changes,
(2010)80(1)97 – 105
Heba M . Elsabba ,Development and growth of mandible – Oral biology
A S MONI ,Anatomy -.
#4 When the skull is observed purely as a bony structure, there is nothing anatomically holding the rest of the skull and mandible together
#7 6 arches develop but 5th arch disappears. These arches are separated by 4 branchial grooves. Each of these five arches contain :
1. A central cartilage rod that forms the skeleton of the arch.
2. A muscular component termed as branchiomere.
3. A vascular component.
4. A neural element.
#8 • The maxillary process becomes the maxilla (or upper jaw), and palate while
the mandibular process from both the sides grow towards each other and fuse in midline at the symphysis.
• The first structure to develop in the primordium of the lower jaw is the
mandibular division of trigeminal nerve
#9 In human beings Meckel’s cartilage has close positional relationship to the developing mandible but makes no contribution to it .
#11 1st the mandibular division of trigeminal nerve develops and around that mesenchymal condensation occurs forming the 1st branchial arch.
Neurotrophic factors produced by the nerve Induce osteogenesis in the ossification centers.
#14 Extension away from the meckels cartilage forms the ramus.
Extension anteriorly forms symphysis region
Ossification around inf alveolar nerve forms inferior alveolar canal
#27 Body of mandible- displacement of ramal bone results in conversion of former ramal bone into posterior part of body of mandible.
In this manner body of mandible lengthens.
#31 In infancy it is usually under-developed. As the age advances the growth of chin becomes significant.
It is influenced by sexual and specific genetic factors.
Males have prominent chins compared to females.
#32 The growth of this cartilage contributes to:
Increase in height of the mandibular ramus
Increase in the over all length of the mandible
Increase of the inter condylar distance
#35 The inferior alveolar artery runs downwards and forwards medial to the ramus of the mandible to reach the mandibular foramen.
Passing through this foramen the artery enters the mandibular canal (within the body of the mandible) in which it runs downwards and then forwards.
Before entering the mandibular canal the artery gives off a lingual branch to the tongue; and a mylohyoid branch that descends in the mylohyoid groove (on the medial aspect of the mandible) and runs forwards above the mylohyoid muscle.
Within the mandibular canal the artery gives branches to the mandible and to the roots of the each tooth attached to the bone. It also gives off a mental branch that passes through the mental foramen to supply the chin.
#37 From the main trunk
a) Meningeal branch/nervous spinosus
b) Nerve to medial pterygoid
From the anterior trunk
a) Buccal nerve (Sensory root)
b) Masseteric
c) Deep temporal
d) Nerve to lateral pterygoid
From the posterior trunk
a) Lingual
b) Auriculo temporal
c) Inferior alveolar nerves
#39 Muscles of tongue- genioglossus
Muscles of pharynx- sup constrictor
Muscles of neck- deep cervical fascia
#41 Mandible shows
D1and D2 bone-It usually seen in anterior mandible.
D2 bone-It is seen in 2/3rds of the time.
D2 bone-It is seen in one half of the patients in posterior mandible.
D3 bone-Remaining one half of patients usually show D3 bone in posterior mandible.
#43 Branches of the inferior alveolar nerve commonly run through these extra foramina and can confer a risk for inadequate anesthesia during surgical procedures involving the mandible
#44 This is a genetic condition that is inherited in an autosomal dominant fashion and found more frequently in the male population
#49 Maxillary teeth are generally directed downward and outward, so bone reduction generally is upward and inward.
Because the mandible is wider at its inferior border than at the residual alveolar ridge in the posterior part of the mouth, resorption, in effect, moves the left and right ridges progressively farther apart.

![REFERENCES
B.D.chaurasia Text book of anatomy vol 3 HEAD AND NECK.
Zarb , bolender, carlson – BOUCHER’S prosthodontic treatment for edentulous
patients,12th
edition
Inderbir singh ,Human anatomy – 7th
edition.
S.I. Bhalajhi, Orthodontics- arts and sciences.
A K Datta ,Human anatomy head and neck .
Nafis Ahmed Faruqi. Human osteology-[clinical orientation]
YI – Pingliu ; Peter – mandibular development , remodelling and age changes,
(2010)80(1)97 – 105
Heba M . Elsabba ,Development and growth of mandible – Oral biology
A S MONI ,Anatomy -.](https://image.slidesharecdn.com/developmentofmandible-250919054802-4fb9f1ad/75/Development-of-Mandible-AND-ITS-IMPORTANCE-58-2048.jpg)