Download as PDF, PPTX

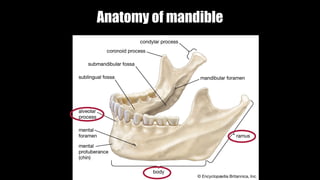
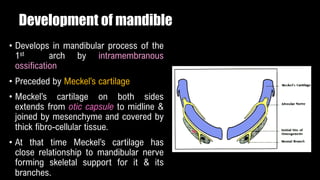
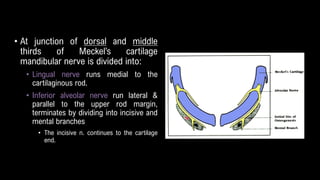
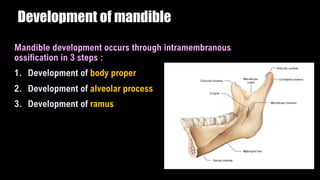
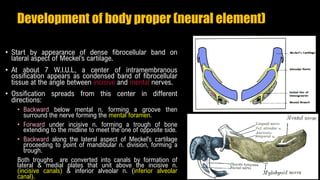
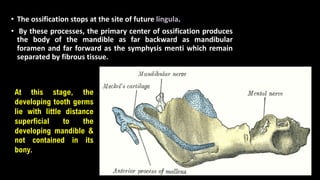
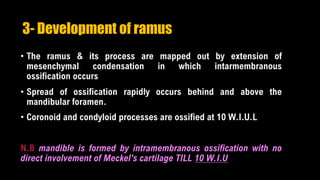
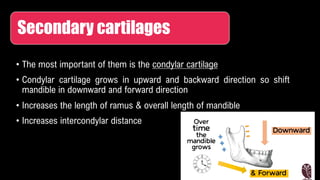
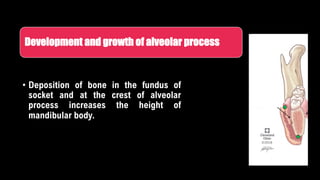
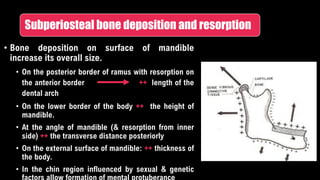
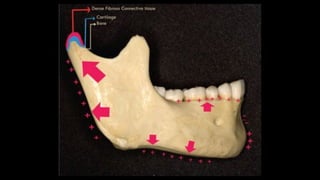
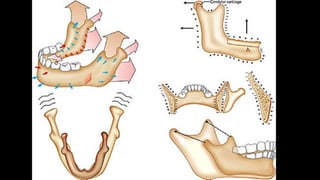

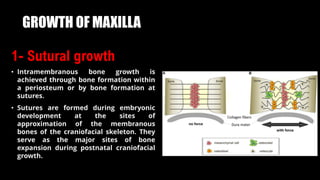
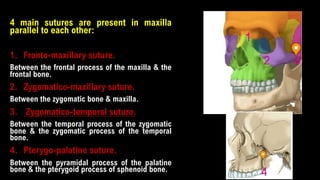
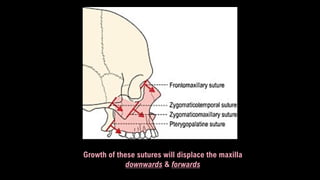
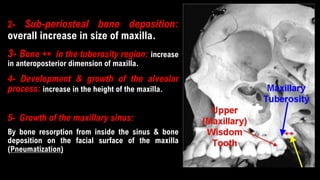



The document details the developmental processes of the mandible and maxilla, explaining that the mandible forms by intramembranous ossification and is influenced by Meckel’s cartilage. It outlines the stages of mandible development, including the body proper, alveolar process, and ramus, emphasizing the role of secondary cartilage and bone deposition in growth. For the maxilla, it describes its formation from two bones and the effects of sutural growth and various bone deposition methods on its size and shape.















































