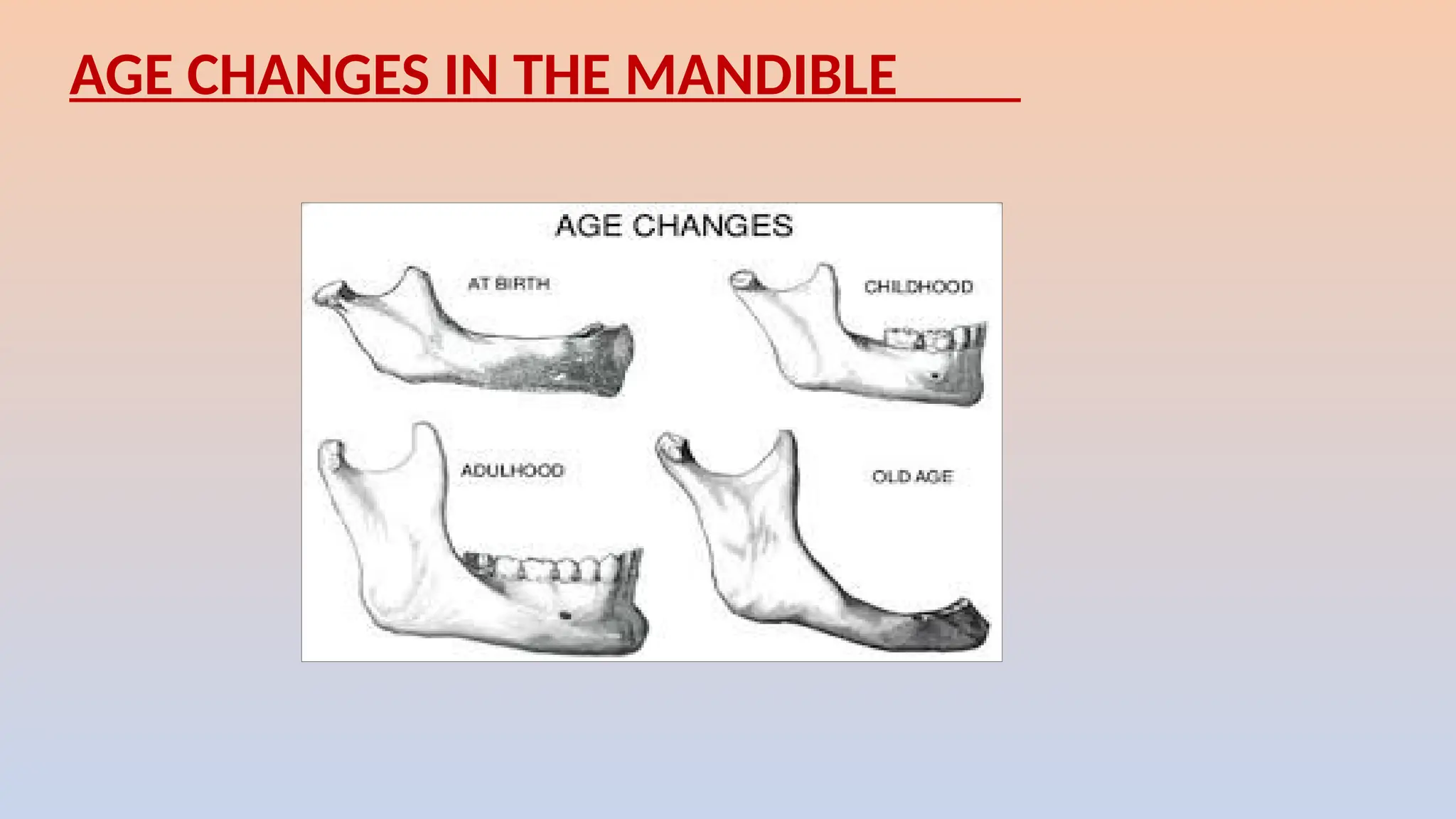
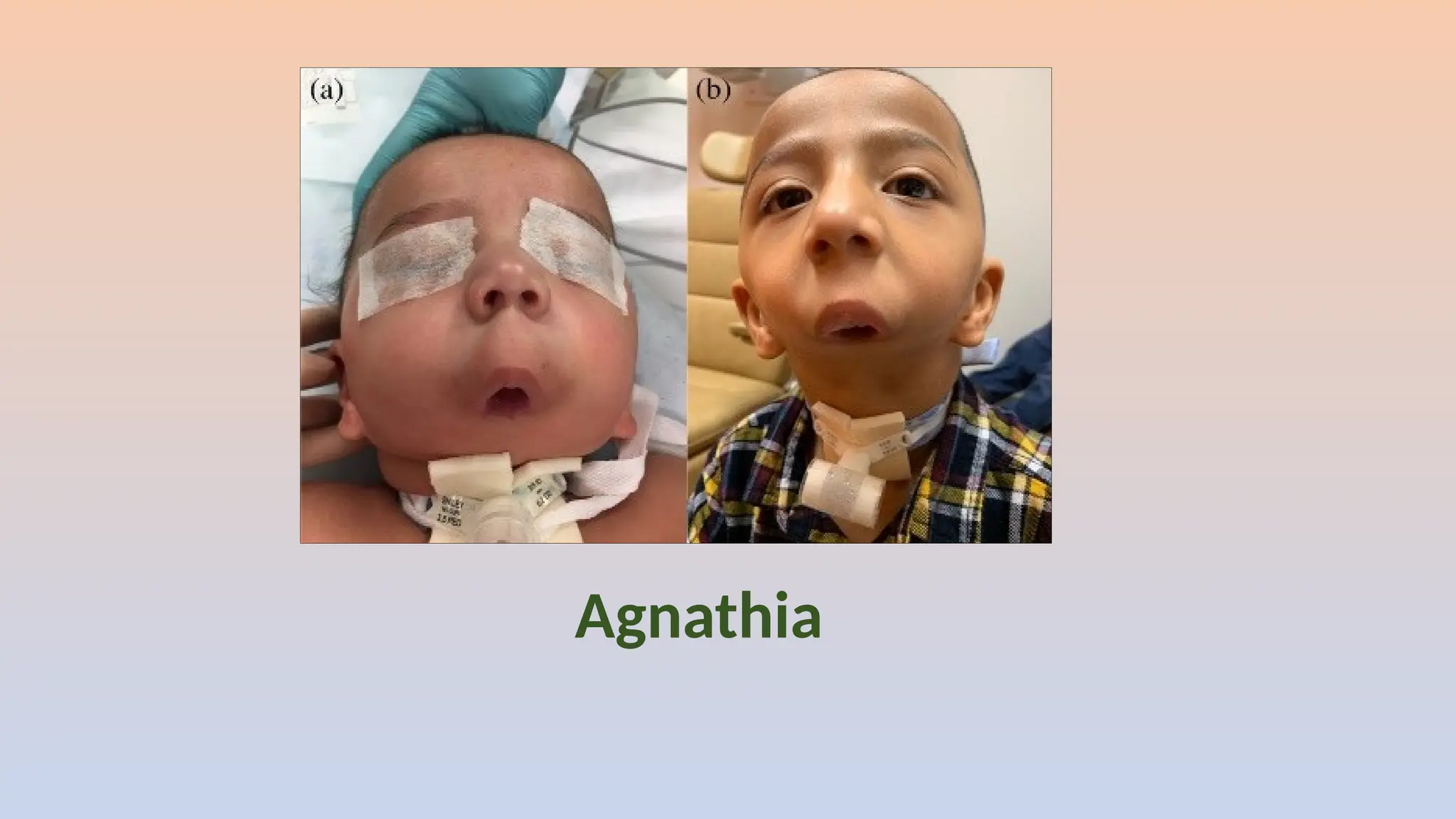
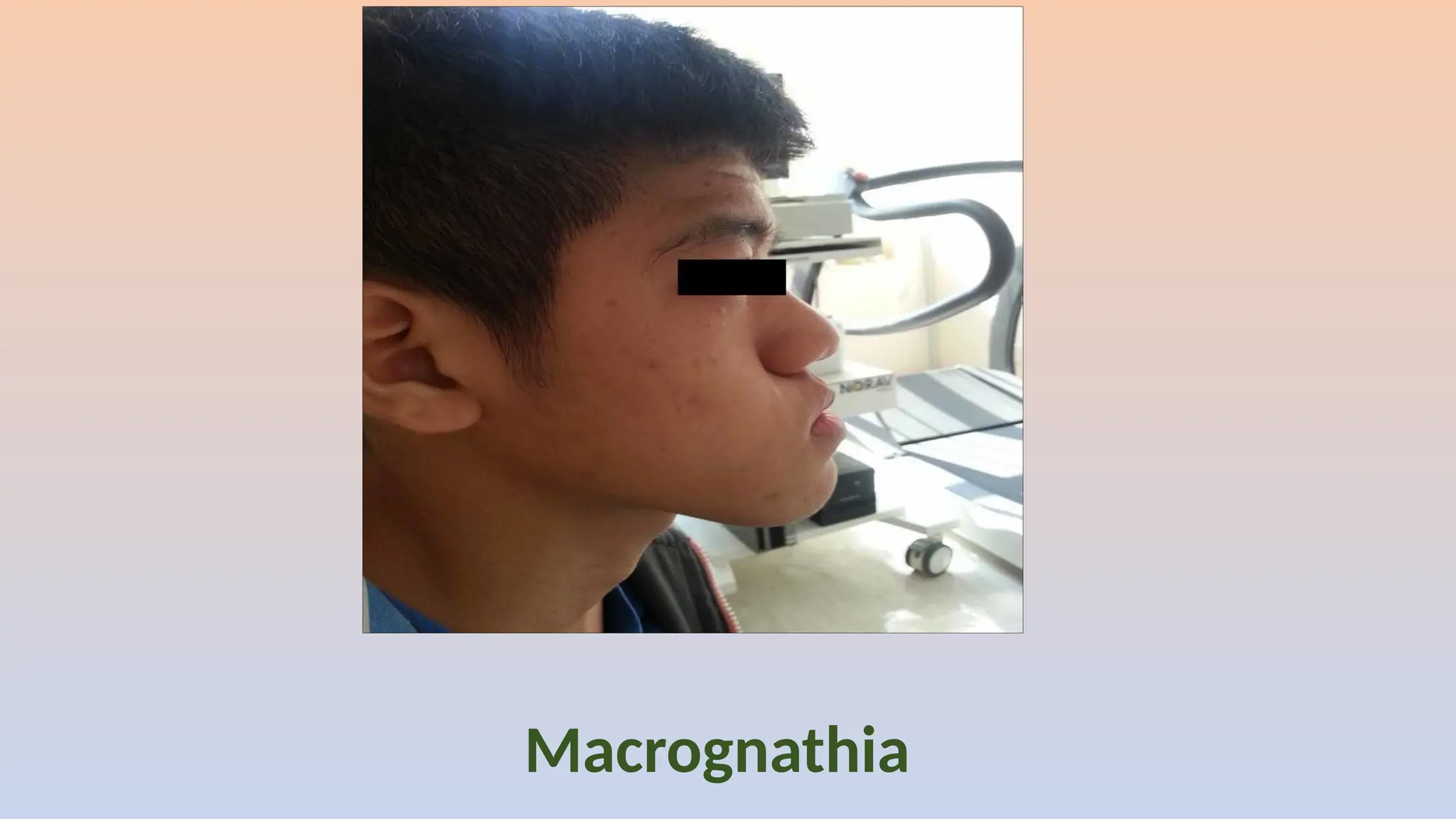
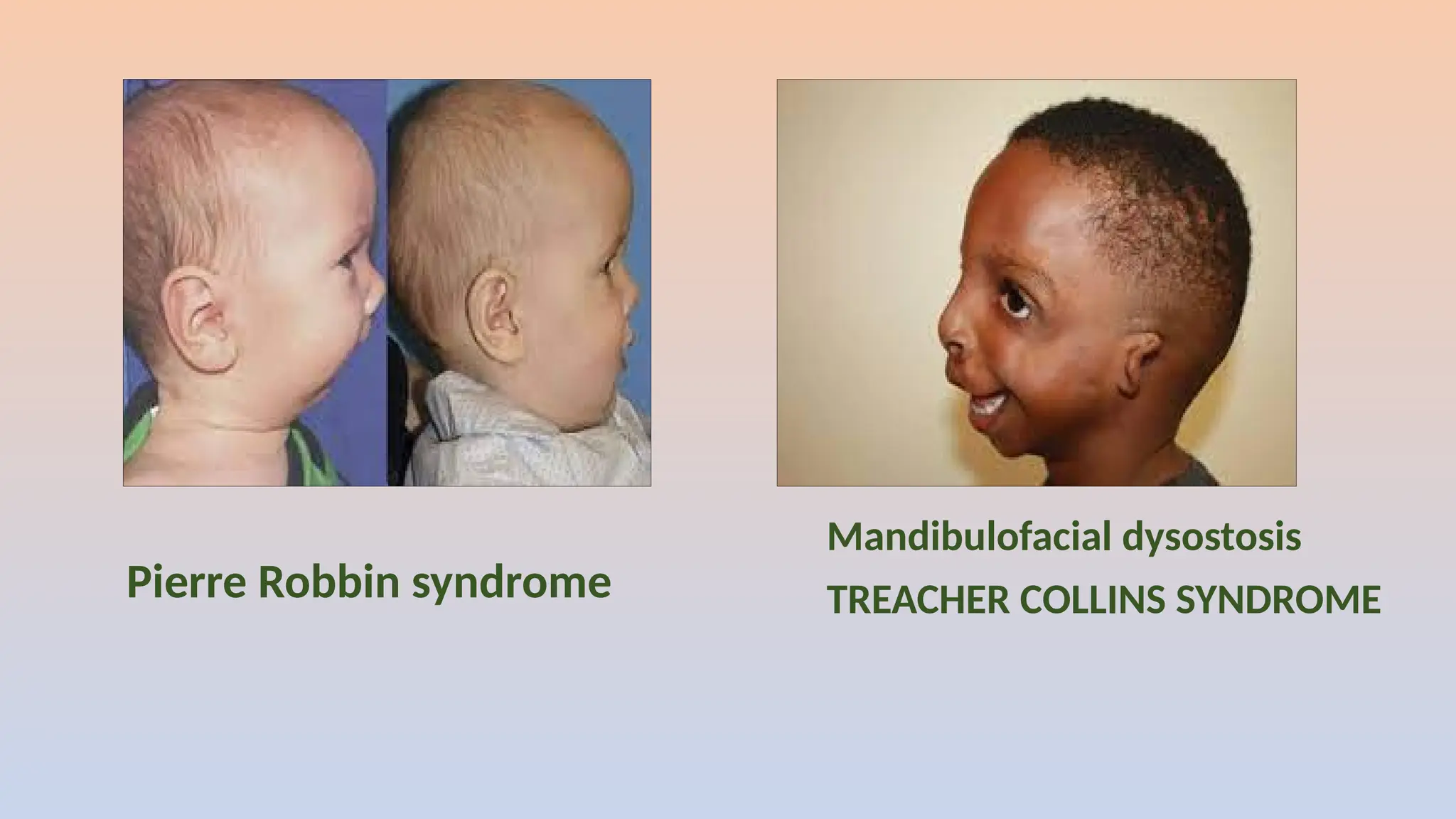
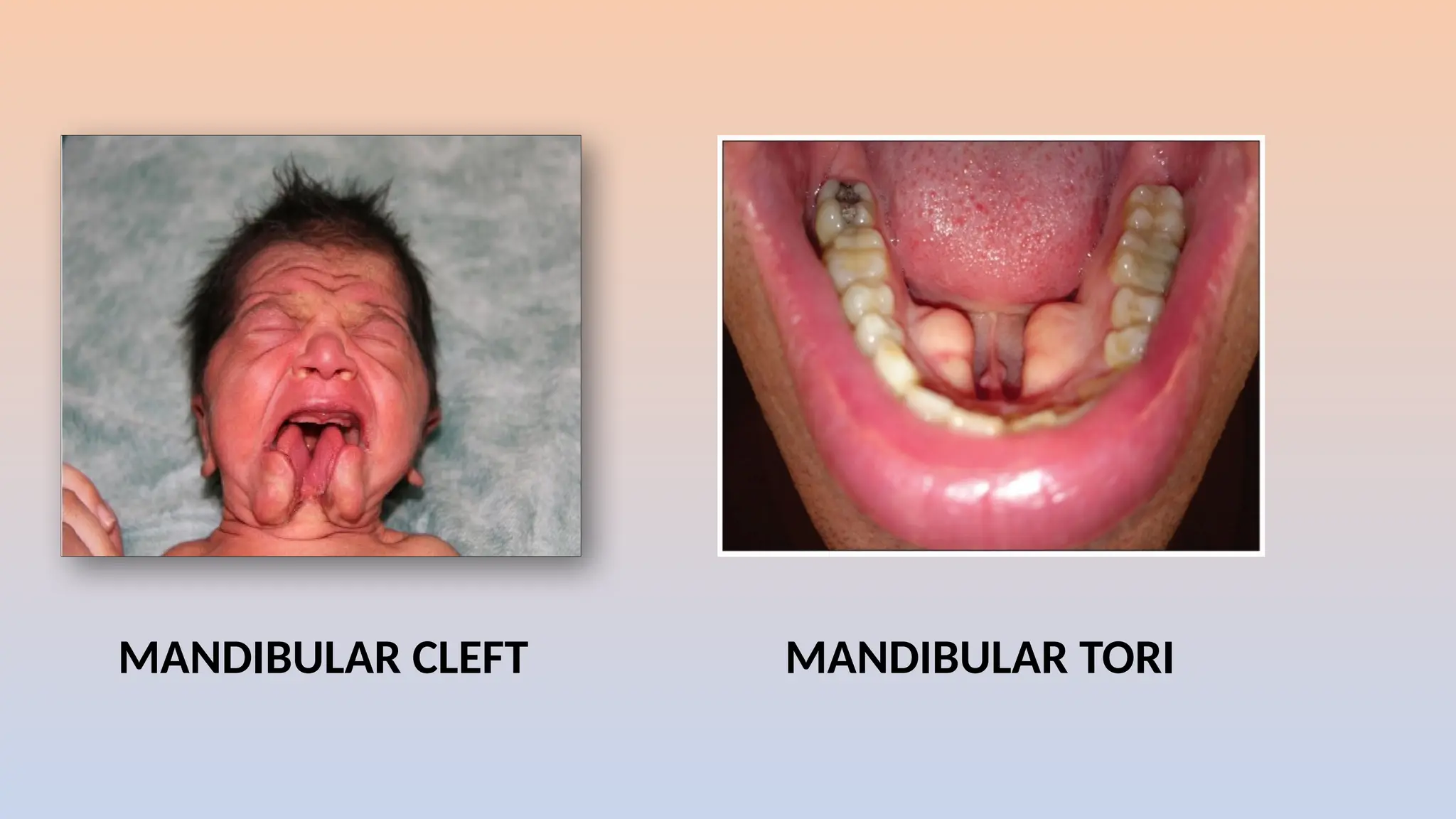
The document discusses the prenatal and postnatal growth and development of the mandible, outlining its anatomy, evolutionary background, and the processes involved in its formation. It details stages of growth during fetal life and infancy, highlighting key changes to the mandible's structure and function influenced by various factors. Additionally, it addresses age-related changes and specific anomalies that can occur in mandibular development.






































































![ORTHODONTIC ARCHWIRES-DR RAKSHITHA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/orthodonticarchwires-drrakshithaautosaved-241223121317-bba0a1ff-thumbnail.jpg?width=640&height=640&fit=bounds)





















