Downloaded 51 times

























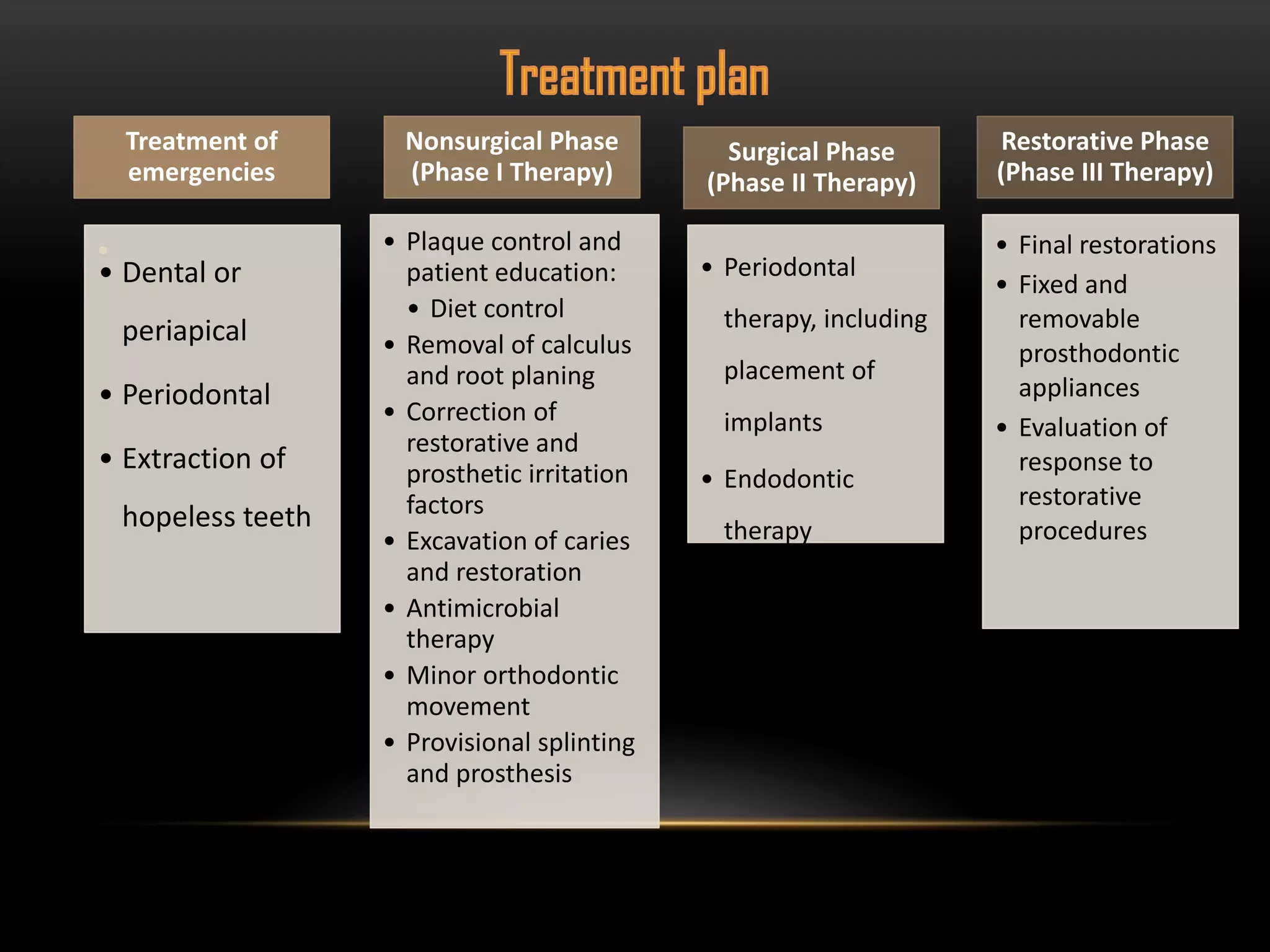


























Nadine Hassan, a 46-year-old Lebanese housewife, presented with pain and a bad smell when chewing on her old bridge. She wanted to fix her teeth and have a beautiful smile. Her medical history included an allergy to penicillin. Her dental history showed multiple extractions due to decay and pain, root canals, and a bridge. Her oral exam found poor hygiene, decay, failed restorations, and mild to moderate periodontitis. Her treatment plan involved emergency extractions, nonsurgical treatments like cleanings and restorations, surgical treatments like extractions and a sinus lift, and restorative treatments like crowns, bridges, and implants.