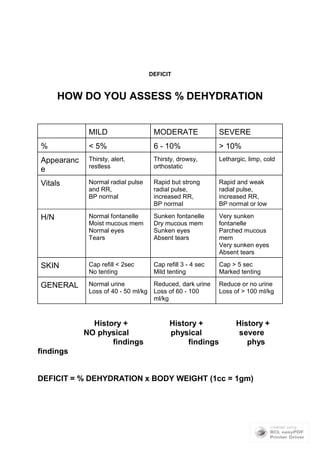
This document provides guidance on pediatric dehydration. It discusses the pathophysiology of different types of dehydration, including isotonic, hypotonic, and hypertonic dehydration. It also outlines the five point assessment of dehydration including volume deficit, electrolyte disturbances, acid-base status, renal function, and potassium levels. Guidelines are provided on oral and intravenous rehydration based on the type and severity of dehydration. The management involves phases of fluid resuscitation and replacement tailored to the individual patient's dehydration status and electrolyte abnormalities.


![PATHOPHYSIOLOGY
Isonatremic (Isotonic) Dehydration: 80%
[Na] between 130 - 150
Roughly equal losses of Na and water
NO change in body tonicity or redistribution of fluid between extra and
intravascular spaces
Hyponatremic (hypotonic) Dehydration: 5%
[Na+] is < 130 mmol/L
Sodium loss > water loss
Most common cause is sodium poor replacement of GI loss
Child appears relatively more ill than expected b/c water shifts from ECF
to ICF :. there is less intravascular volume and more physical signs
Na < 120: seizures, coma
Cerebral edema can lead to seizures
Hypo-osmolar demyelination syndrome,most commonly seen as
central pontine myelinolysis, can occur. Uncertain whether these are
due to hyponatremia itself or too rapid correction of Na+. Pathophysiology
unknown. Thought to be due to rapid correction in chronic hyponatremia.
Neurological findings include fluctuating LOC, behavioral disturbances,
convulsions progressing to pseudobulbar palsy and quadraparesis.
Hypernatremic (Hypertonic) Dehydration: 15%
[Na+] > 150 mmol/L
Water loss > sodium loss or increased Na+ intake (incorrect formulas)
Child appears relatively less ill than it is b/c water shifts from ICF to ECF :.
there is more relative intravascularvolume and less physical signs
Risk: brain hemorrhage, SZ, coma, death
Do NOT correct rapidly w/ hypotonic solution b/c of brain shifts which can
cause massive brain swelling
May have alternating LOC b/w lethargy and hyperirritability
PE: dry, rubbing, doughy skin w/ inc muscle tone (doughy skin b/c
hypertonicity of body fluids in subcutaneous tissues)
Risk: intracellular dehydration :. water shifts out of the brain cells. This
stress causes production of idiogenic osmols (glycine and taurine) which
prevents ongoing water loss from neurons. If serum Na is lowered too
quickly, these idiogenic osmols will then attract water into brain cells
causing swelling, massive cerebral edema, and intractable seizures.
MUST correct serum Na slowly, and remember that tissue/renal
perfusion is maintained w/ high Na
MANAGEMENTOF SEVERE DEHYDRATION
Approach is ABCs with emphasis on iv access
ALL types of severe dehydration require a fluid bolus of 20 cc/kg of 0.9% NaCl or
Ringers
Theoretical risk of acidosis with normal saline: infusion of NaCl dilutes the extracellular
HC03- creating a “dilutional acidosis”. Ringers lactate has some HCO3 in it.
Reassess q 5-10 min after bolus and repeat as needed X 2
Avoid glucose containing solutions for initial resuscitation of severe dehydration
If hypoglycemic: give 2ml/kg D25W (children) or 4ml/kg DW10 (infants)if hypoglycemic
Consider colloids (albumin, FFP, synthetics) if renal, cardiac, or pulmonary dz
Consider differential dx of shock if nonresponsive to 3 boluses (>60 ml/kg): septic, spinal,](https://image.slidesharecdn.com/dehydration-150429153411-conversion-gate02/85/Dehydration-3-320.jpg)
![hypovolemic, hemorrhagic, obstructive, cardiogenic, anaphylactic, other
ISONATREMIC DEHYDRATION
Phase I (0 - 20min): Bolus 20 cc/kg X 3 prn of normal saline, lactate ringers
Phase II (0 - 8hrs): Infusion with D5W 0.45% normal saline (D5W ½ NS)
Add 20 mEq/L KCL after urine output established
Rate cc/hr = (½ deficit - bolus) + maintenance X 8hrs + ongoing losses
8 hours
Phase III (8-24hrs): Infusion with D5W 0.45%NS
Adjust according to urine output if neccessary; monitor lytes
Rate cc/hr = ½ deficit + maintenance X 16hrs + ongoing losses
16 hours
HYPONATREMIC DEHYDRATION
Phase I (0-20min): Bolus 20 cc/kg X 3 prn of NS or LR
Phase II (0-8hrs)
If not seizing ...
- administer D5W ½ NS with objective to raise serum Na by
no more than 12 mEq/L over 24hrs
- no NaCl bolus necessary
- rate cc/hr = (½ deficit - bolus) + maintenanceX8hrs +
losses 8 hours
If seizing...
- Na deficit = (desired - current [Na]) X TBW X weight (kg)
- Na deficit = (120 - [Na]) X 0.6 X kg
- replace with 3% saline (0.5 mEq/ml or 513 mEq/L)
- use 120 as desired Na to prevent rapid overcorrection
- proceed with fluids to raise Na by no more than 12 mEq/L
over next 24hrs; monitor lytes
- after 3% saline, use D5W ½ NS
- rate cc/hr = (½ deficit - bolus) + maintenanceX8hrs +
losses 8 hours
Phase III (8-24hrs)
DW5 ½ NS
Rate cc/hr =1/2 deficit + maintenance X 16hrs + ongoing losses
16 hours
HYPERNATREMIC DEHYDRATION
Phase I: Bolus 20 cc/kg NS X 3 prn
Phase II/III
Treat shock and give fluids to replace deficits over 48hrs (vs 24hr)
Reduce serum Na by no more than 10 mEq/L/24hrs
Dialysis for SeNa > 210 mEq/L
Acceptable solutions: D5W0.45%NS or D5W0.2%NS
NOTE that rate of solution more important than type of solution
Rate cc/hr = (½ deficit - bolus) + maintenanceX24hrs + ongoing losses
24 hours
SPECIAL SITUATIONS](https://image.slidesharecdn.com/dehydration-150429153411-conversion-gate02/85/Dehydration-4-320.jpg)










































![Dehydration [Autosaved].vghvcghjjvvgpptx](https://cdn.slidesharecdn.com/ss_thumbnails/dehydrationautosaved-250909163637-53a99fcc-thumbnail.jpg?width=640&height=640&fit=bounds)
































