Downloaded 93 times



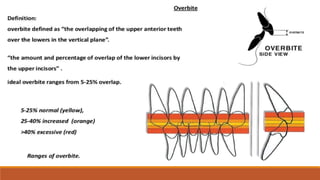





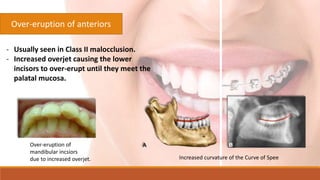





The document discusses deep bite, a type of dental malocclusion characterized by excessive overlapping of the lower incisors by the upper ones. It outlines various causes, including genetic factors and dental issues, and presents treatment options ranging from removable appliances to orthognathic surgery, especially for severe cases. It highlights the importance of addressing deep bites due to their prevalence and the potential need for specialized correction methodologies.






























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)











