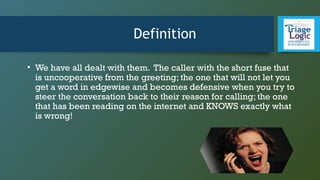
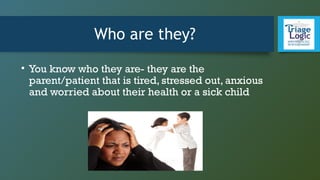
This document provides guidance on dealing with difficult callers for triage nurses. It defines difficult callers as tired, stressed, anxious parents calling about a sick child. These callers are not targeting the nurse personally but are at the end of their rope. The document advises nurses to listen to callers vent for a few minutes, show empathy, and avoid arguing. It provides guidelines for angry, demanding, and overly worried callers that focus on de-escalation, clarifying needs, offering solutions, documenting objectively, and involving physicians if needed.