Downloaded 86 times

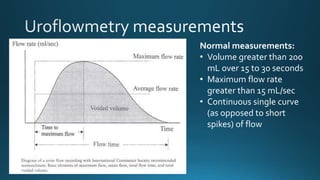

This document discusses normal bladder function measurements including a volume greater than 200 mL over 15 to 30 seconds, a maximum flow rate greater than 15 mL/sec, and a continuous single curve of flow as opposed to short spikes.