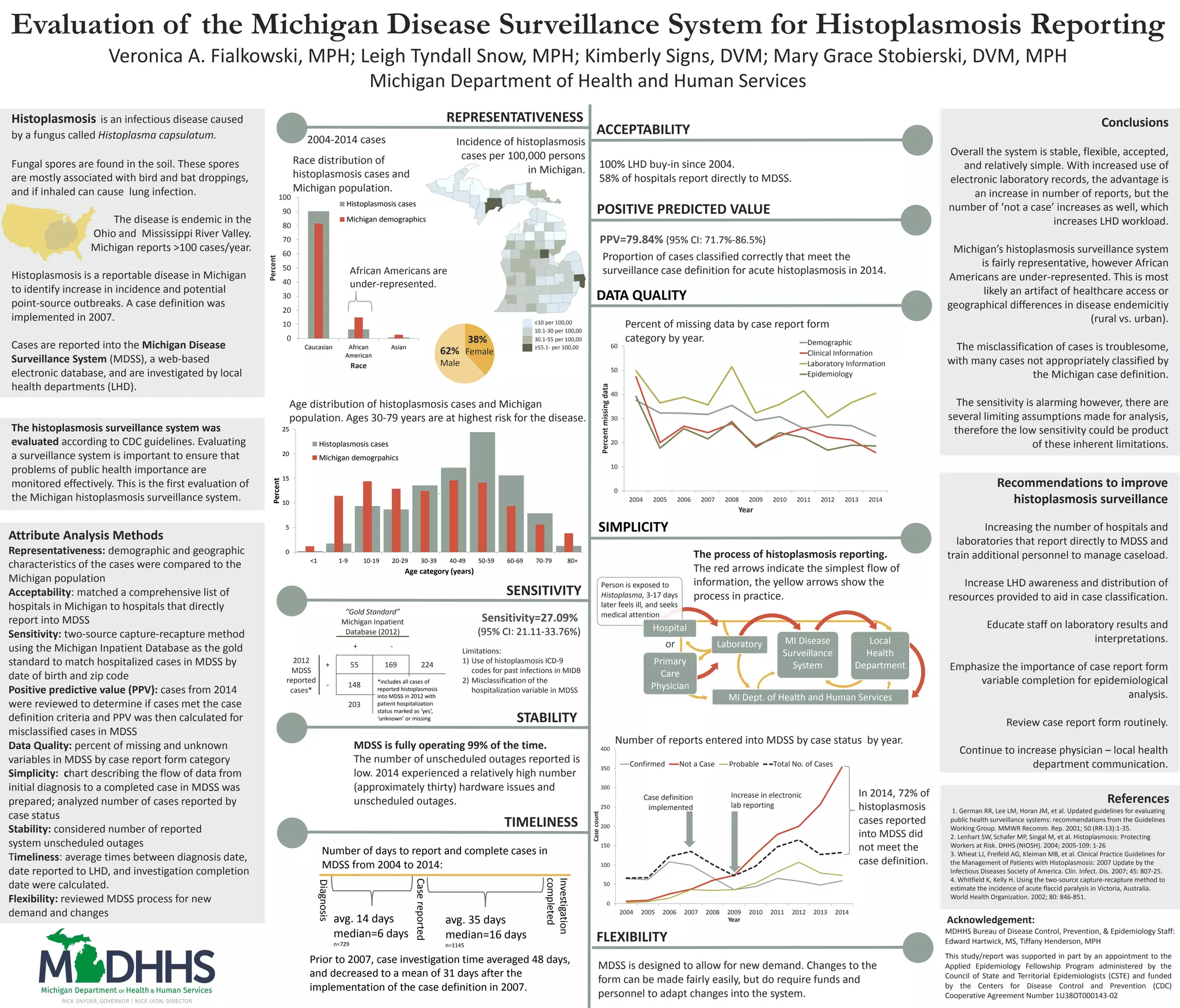
The Michigan Disease Surveillance System for histoplasmosis reporting was evaluated according to CDC guidelines. Several key findings were:
1) The system was found to be stable, flexible, and relatively simple to use, though the sensitivity was low at 27.09% and misclassification of cases was high.
2) Reporting timeliness improved after a 2007 case definition implementation, with investigation completion times decreasing from 48 to 31 days on average.
3) The system was fairly representative though underrepresented African Americans; recommendations were made to improve case classification and data quality.










![Meghaan Walsh HJS Poster[1]](https://cdn.slidesharecdn.com/ss_thumbnails/7022ecd4-42b6-48cb-bf38-4a4927082be4-160811165238-thumbnail.jpg?width=640&height=640&fit=bounds)




































