History Of RandomizedTrials
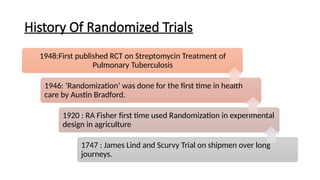
1948:First published RCT on Streptomycin Treatment of
Pulmonary Tuberculosis
1946: ‘Randomization’ was done for the first time in health
care by Austin Bradford.
1920 : RA Fisher first time used Randomization in experimental
design in agriculture
1747 : James Lind and Scurvy Trial on shipmen over long
journeys.
6.
6
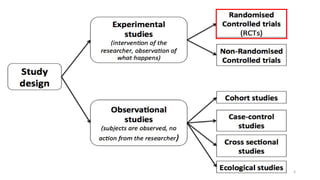
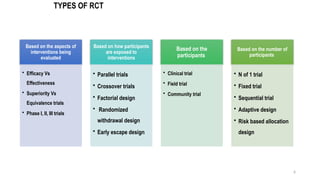
TYPES OF RCT
Basedon the aspects of
interventions being
evaluated
• Efficacy Vs
Effectiveness
• Superiority Vs
Equivalence trials
• Phase I, II, III trials
Based on how participants
are exposed to
interventions
• Parallel trials
• Crossover trials
• Factorial design
• Randomized
withdrawal design
• Early escape design
Based on the
participants
• Clinical trial
• Field trial
• Community trial
Based on the number of
participants
• N of 1 trial
• Fixed trial
• Sequential trial
• Adaptive design
• Risk based allocation
design
7.
7
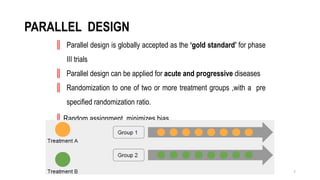
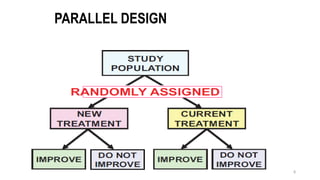
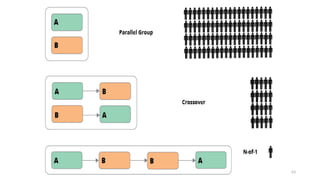
PARALLEL DESIGN
║ Paralleldesign is globally accepted as the ‘gold standard’ for phase
III trials
║ Parallel design can be applied for acute and progressive diseases
║ Randomization to one of two or more treatment groups ,with a pre
specified randomization ratio.
║Random assignment minimizes bias
CROSS OVER TRIAL
•A crossover design is a modified randomized block design in which each block receives >1
treatment at different dosing periods.
• A block can be a patient or a group of patients. Patients in each block receive different
sequences of treatments.
• A crossover design is called a complete crossover design if each sequence contains all
treatments under investigation.
10.
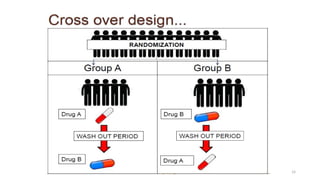
2. Crossover StudyDesign
• As the previous type , the participants are randomly assigned to a study &
control group followed by a washout period, and then followed by switching
or exchange of study and control group.
• There must be enough of washout period for weaning off from the effects
of both the interventions.
• The subjects act as their own control in this kind of study.
• Fewer subjects are required compared to parallel study design.
• Planned crossovers are not possible in case of surgical interventions or if
the new intervention completely cures the disease.
• Not helpful in acute conditions.
12
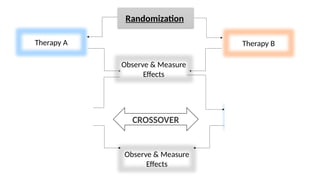
CROSS OVER TRIAL
Subjectsare initially randomly allocated into therapy ‘A’ or therapy ‘B’
After being observed for a certain period of time the subjects are given a period of “wash -
out” to remove the existing effects of therapy.
The subjects are switched over to the other therapy (Cross over) and are thereafter again
followed up for another relevant period of time
13.
13
CROSS OVER TRIAL
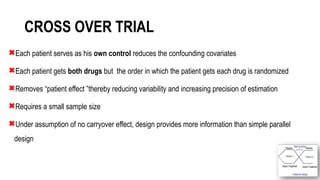
Eachpatient serves as his own control reduces the confounding covariates
Each patient gets both drugs but the order in which the patient gets each drug is randomized
Removes “patient effect ”thereby reducing variability and increasing precision of estimation
Requires a small sample size
Under assumption of no carryover effect, design provides more information than simple parallel
design
Crossover designs maybe used in clinical trials in the following
situations where
1. Objective measures and interpretable data for both efficacy and
safety are obtained.
2. Chronic (relatively stable) disease are under study.
3. Prophylactic drugs with relatively short half-life are being
investigated.
4. Relatively short treatment periods are considered.
5. Baseline and washout periods are feasible.
17.
17
PRE REQUISITES OFCROSS OVER DESIGN
Disease – chronic (asthma, osteoarthritis) stable
Drugs with relatively short half-life & short treatment periods are considered
Effects of drug should develop fully within treatment period
Washout periods -sufficiently long for complete reversibility of drug effect
Wash out period- five half lives of drug
18.
18
• Treatment sequencingand patient assignment: The sequence in which treatments are administered
should ideally be assigned randomly. This protects against conscious and unconscious bias by ensuring
that there are no systematic differences between patients receiving A/B versus B/A.
• Crossover rules and timing of measurements:
Time-dependent -the treatment switch takes place after a specified length of time),
Disease-state dependent -the treatment switch is determined by the clinical characteristics of the patient
These crossover points should be concealed from both patients and observers in order to reduce the
influence of carryover effects and period effects
19.
High-dose Valacyclovir DecreasesPlasma HIV-1 RNA
More Than Standard-dose Acyclovir in HIV-1, HSV-2
Positive Persons: a Randomized, Crossover Trial.
J Acquir Immune Defic Syndr. 2013 Jun 1; 63(2): 201–208.
• Valacyclovir 1000 mg twice daily or Acyclovir 400 mg
twice daily for 12 weeks, followed by a two week
washout
• HSV DNA was measured from daily self-collected genital
swabs for the initial 4 weeks of each arm and HIV-1 RNA
was quantified from weekly plasma samples
• High-dose valacyclovir reduces plasma HIV-1 RNA levels
more than standard-dose acyclovir in HIV-1/HSV-2
seropositive persons not receiving antiretroviral therapy
20.
1b. Cross overdesign
• Strengths
• Smaller sample size than parallel groups
• Results depending only on within patient variability
• Often used in healthy volunteers (for phase 1 clinical trials)
• Limitations
• Only in stable chronic diseases
• Endpoint must not be sensitive to learning processes.
• Requires a wash-out period between treatment periods.
• Long follow-up
• Analysis must confirm the absence of treatment - period interaction
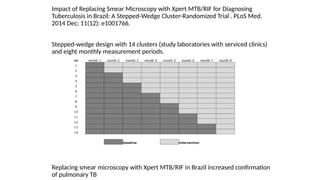
Impact of ReplacingSmear Microscopy with Xpert MTB/RIF for Diagnosing
Tuberculosis in Brazil: A Stepped-Wedge Cluster-Randomized Trial . PLoS Med.
2014 Dec; 11(12): e1001766.
Stepped-wedge design with 14 clusters (study laboratories with serviced clinics)
and eight monthly measurement periods.
Replacing smear microscopy with Xpert MTB/RIF in Brazil increased confirmation
of pulmonary TB
27.
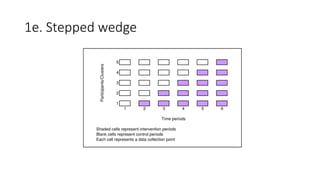
1e. Stepped wedge
Strengths:
•Efficiency: Units act as their own control, so fewer units needed
(same as cross-over design)
• Power is relatively insensitive to Coefficient of variation
• Power can be maximize the number of steps
• Logistical or financial - cannot introduce the intervention in all
units at once
• Evaluate the community effectiveness of an intervention
previously shown to be efficacious in an individually
randomized trial or in a different setting
• Systematically evaluate new program
• To study the effect of time on intervention effectiveness (i.e.
seasonality, time since introduction)
28.
1e. Stepped wedge
Limitations
•Intervals should be long enough to capture the full treatment effect
• Multiple data collection points required
• Effect of variation with time
• Complex data analysis
29.
Commonly used crossover designs
Commonly used cross over designs in bioavailability trails are
Latin square cross over design
Balanced incomplete block design
Replicate Crossover-study design
30.
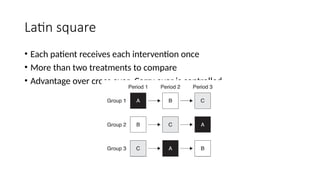
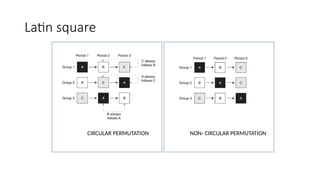
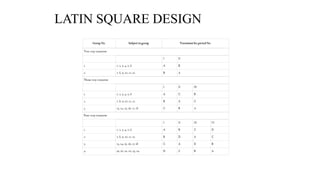
LATIN SQUARE DESIN
•The Latin-square design plans the clinical trial so that each subject
receives each drug product only once, with adequate time between
medications for the elimination of the drug from the body.
• In this design, each subject is his own control, and subject-to-subject
variation is reduced.
• Moreover, variation due to sequence, period, and treatment
(formulation) are reduced, so that all patients do not receive the same
drug product on the same day and in the same order.
• Possible carryover effects from any particular drug product are
minimized by changing the sequence or order in which the drug
products are given to the subject.
• Thus, drug product B may be followed by drug product A, D, or C .
• After each subject receives a drug product, blood samples are collected
at appropriate time intervals so that a valid blood drug level–time curve
is obtained.
31.
CONTI…
• The timeintervals should be spaced so that the peak blood concentration, the total
area under the curve, and the absorption and elimination phases of the curve may
be well described.
• The crossover design is a type of Latin square. In a Latin square the number of
treatments equals the number of patients.
• In addition, another factor, such as order of treatment, is included in the
experiment in a balanced way.
• The net result is an N X N array (where N is the number of treatments or patients)
of N letters such that a given letter appears only once in a given row or column.
This is most easily shown pictorially.
32.
Two-Period Crossover Design
•For randomizations of treatments in Latin squares, For the comparison of two formulations, a 2 X
2 Latin square (N = 2) consists of two patients each taking two formulations (A and B) on two
different occasions in two “orders”.
• The balancing of order (A-B or B-A) takes care of time trends or other ‘‘period’’ effects, if present.
(A period effect is a difference in response due to the occasion on which the treatment is given,
independent of the effect due to the treatment).
• The 2 X 2 Latin square shown above is familiar to all who have been involved in
bioavailability/bioequivalence studies. In these studies, the 2 X 2 Latin square is repeated several
times to include a sufficient number of patients. Thus the crossover design can be thought of as a
repetition of the 2 X 2 Latin square.
33.
CONTI...
• 2 formulations,even number of subjects, randomly divided into 2 equal groups.
• First period , each member of one group receive a single dose of the test
formulation; each member of the other group receive the standard formulation.
• After a wash period (5 half lives), in second period , each member of the
respective groups will receive an alternative formulation & experiment will be
repeated.
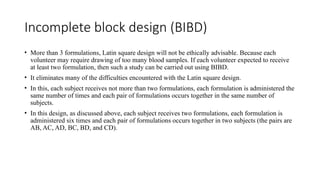
Incomplete block design(BIBD)
• More than 3 formulations, Latin square design will not be ethically advisable. Because each
volunteer may require drawing of too many blood samples. If each volunteer expected to receive
at least two formulation, then such a study can be carried out using BIBD.
• It eliminates many of the difficulties encountered with the Latin square design.
• In this, each subject receives not more than two formulations, each formulation is administered the
same number of times and each pair of formulations occurs together in the same number of
subjects.
• In this design, as discussed above, each subject receives two formulations, each formulation is
administered six times and each pair of formulations occurs together in two subjects (the pairs are
AB, AC, AD, BC, BD, and CD).
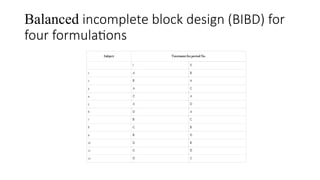
Replicate Crossover-study design
•For highly variable drugs.
• It allows comparisons of within-subject variances.
• It reduces the number of subjects needed.
• Four-period, two-sequence, two-formulation design
(recommended) or Three-sequence, three-period, single-
dose, partially replicated.
• Replicated crossover designs are used for the determination
of individual bioequivalence, to estimate within-subject
variance for both the Test and Reference drug products, and
to provide an estimate of the subject-by-formulation
interaction variance.
• Generally, a four-period, two-sequence, two-formulation
design is recommended by the FDA.
38.
PERIOD 1 23 4
GROUP 1 T R T R
GROUP 2 R T R T
Where,
R = reference
T = treatment
The same reference and the same test are each given twice to the same
subject. Other sequences are possible. In this design, Reference-to-
Reference and Test-to-Test comparisons may also be made.
39.
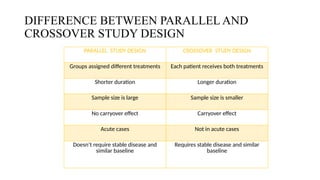
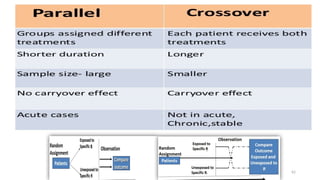
DIFFERENCE BETWEEN PARALLELAND
CROSSOVER STUDY DESIGN
PARALLEL STUDY DESIGN CROSSOVER STUDY DESIGN
Groups assigned different treatments Each patient receives both treatments
Shorter duration Longer duration
Sample size is large Sample size is smaller
No carryover effect Carryover effect
Acute cases Not in acute cases
Doesn’t require stable disease and
similar baseline
Requires stable disease and similar
baseline
40.
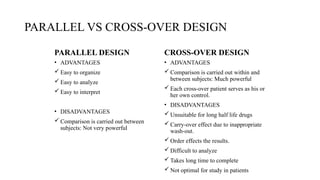
PARALLEL VS CROSS-OVERDESIGN
PARALLEL DESIGN CROSS-OVER DESIGN
• ADVANTAGES
Easy to organize
Easy to analyze
Easy to interpret
• DISADVANTAGES
Comparison is carried out between
subjects: Not very powerful
• ADVANTAGES
Comparison is carried out within and
between subjects: Much powerful
Each cross-over patient serves as his or
her own control.
• DISADVANTAGES
Unsuitable for long half life drugs
Carry-over effect due to inappropriate
wash-out.
Order effects the results.
Difficult to analyze
Takes long time to complete
Not optimal for study in patients
41.
42
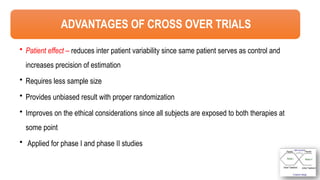
ADVANTAGES OF CROSSOVER TRIALS
• Patient effect – reduces inter patient variability since same patient serves as control and
increases precision of estimation
• Requires less sample size
• Provides unbiased result with proper randomization
• Improves on the ethical considerations since all subjects are exposed to both therapies at
some point
• Applied for phase I and phase II studies
42.
Advantages:
1. It allowsa within-patient comparison between treatments, since
each patient serves as his or her own control.
2. It removes the interpatient variability from the comparison
between treatments.
3. With a proper randomization of patients to the treatment
sequences, it provides the best unbiased estimates for t
43.
44
DISADVANTAGES OF CROSSOVER TRAILS
• Carryover effect-the effect of a treatment in one period may carry over into the next period.
• Period effect- patients vary from one period to another. The disease may naturally
progress, regress, or fluctuate in severity.
• Not useful for acute disease
• Needs to determine appropriate length of washout period
• Blinding – subjects able to compare drugs
• Assessing adverse events
• High dropout rates
• Not suitable for Behavioral/educational interventions
• The order in which the therapies are given may elicit psychological response
44.
1. Carry- overeffects: The residual influence of treatments on subsequent
treatment periods. Avoided by wash out period.
2. Order effects: Order in which the tt are administered affects the outcome.
3. Period effects: The diff. between the study periods.
4. Drop-outs can be higher.
It is the rest period between 2 treatment periods.
• It permits the effect of previous treatment to wane off.
• It should be long enough for the treatment effect to wear off so that there is
no carryover effect of previous treatment to next.
• It depends upon the nature of the drug.
24/03/2025 48
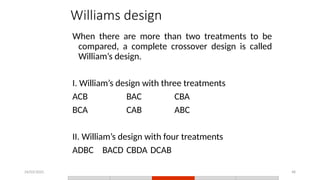
Williams design
Whenthere are more than two treatments to be
compared, a complete crossover design is called
William’s design.
I. William’s design with three treatments
ACB BAC CBA
BCA CAB ABC
II. William’s design with four treatments
ADBC BACD CBDA DCAB
48.
24/03/2025 49
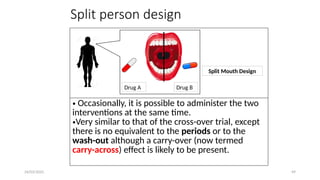
Split persondesign
• Occasionally, it is possible to administer the two
interventions at the same time.
•Very similar to that of the cross-over trial, except
there is no equivalent to the periods or to the
wash-out although a carry-over (now termed
carry-across) effect is likely to be present.
Drug A Drug B
Split Mouth Design
49.
24/03/2025 50
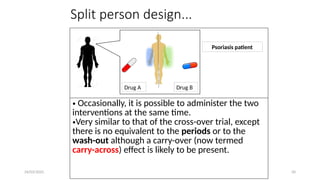
Split persondesign...
Drug A Drug B
Psoriasis patient
• Occasionally, it is possible to administer the two
interventions at the same time.
•Very similar to that of the cross-over trial, except
there is no equivalent to the periods or to the
wash-out although a carry-over (now termed
carry-across) effect is likely to be present.
50.
24/03/2025 51
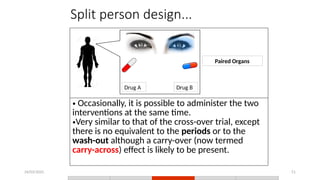
Split persondesign...
• Occasionally, it is possible to administer the two
interventions at the same time.
•Very similar to that of the cross-over trial, except
there is no equivalent to the periods or to the
wash-out although a carry-over (now termed
carry-across) effect is likely to be present.
Drug A Drug B
Paired Organs
53
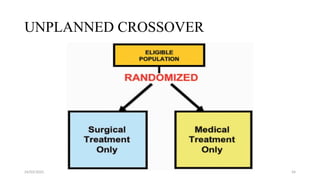
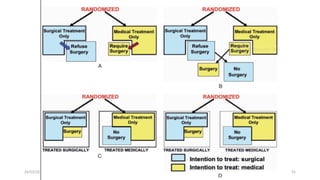
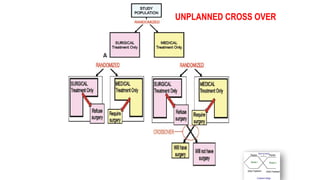
UNPLANNED CROSS OVER
Ina trial to assess the efficacy of surgical Vs medical treatment in IHD
Some patients initially randomly allocated to surgical
or medical options, may start having second thoughts and
may decide to finally take the other form of therapy to which
they were originally not allocated;
or
Some patients initially allocated to medical group may deteriorate and may then be
given surgery. Such crossovers may lead to serious objections as regards the validity
of the trial.
59
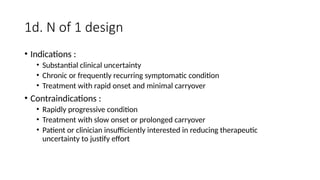
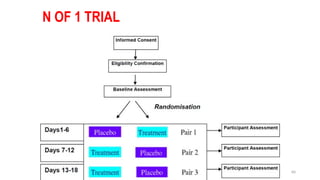
N of 1trial
Multiple crossover trials, usually randomized and blinded, conducted in a single patient.
N-of-1 trials are a specific form of randomized designs characterized by periodic switching
from active treatment to placebo or between active treatments(("withdrawal-reversal"
designs)
Done when there is doubt about whether a treatment is really providing benefit to the
patient.
By prescribing multiple episodes of treatment, n-of-1 trials increase precision of
measurement and control for treatment-by-time interaction
61
SERIAL CONTROLLED N-OF-1TRIALS OF TOPICAL
VITAMIN E AS PROPHYLAXIS FOR CHEMOTHERAPY-
INDUCED ORAL MUCOSITIS IN PAEDIATRIC PATIENTS.
Sung L1
, Tomlinson GA, Greenberg ML, Koren G, Judd P, Ota S, Feldman BM
Researchers evaluated theeffectiveness of the cannabinoid dronabinol on central neuropathic pain in patients with multiple
sclerosis.[1] The effectiveness of cannabinoids in relieving pain caused by central lesions in multiple sclerosis had not been
investigated previously. A randomised double blind placebo controlled crossover trial study design was used. The
intervention was orally administered dronabinol at a maximum dose of 10 mg daily or corresponding placebo. Each treatment
period was for three weeks, separated by a three week washout period. All analgesic drugs, except for paracetamol, were
discontinued at least one week before the start of the trial.
The primary outcome was spontaneous pain intensity in the last week of each treatment period measured using a numerical
rating scale. The researchers reported that, when compared with placebo, dronabinol had a significant analgesic effect on central
pain in patients with multiple sclerosis. Although the effects were modest they were clinically relevant. The number of
patients with adverse events was higher during active treatment, especially in the first week of treatment. The functional ability
of the patients with regard to their multiple sclerosis did not change.
Which of the following statements, if any, are true?
a) All participants received both treatments in the same
sequence order
b) Each participant acted as his or her own control
c) The purpose of the washout period was to allow the effects
of the first treatment to dissipate before starting the second
treatment
d) The crossover study design required more participants
than if a “between subjects” study design had been used to
compare dronabinol and placebo
Editor's Notes
#13 Opportunity to receive both treatments (or be assured of receiving active treatment at some point) is attractive to patients
#26 the order in which the intervention is received is randomised
#42 There is no guarantee that washout periods will completely control for carryover effects.
Long washout periods might unavoidably increase the duration of the experiment.
Ethical concerns (how long can a patient be refused treatment during a washout period) and incomplete knowledge (what washout
period length is sufficient) may sometimes lead to inadequate washout periods.
Within each unit, or patient, responses to therapy are likely to be correlated (eg, a single patient’s response to treatment A is correlated with that patient’s response to treatment B; the responses are not independent). This causes complexities in both the design and the analysis
#44 There is no guarantee that washout periods will completely control for carryover effects.
Long washout periods might unavoidably increase the duration of the experiment.
Ethical concerns (how long can a patient be refused treatment during a washout period) and incomplete knowledge (what washout
period length is sufficient) may sometimes lead to inadequate washout periods.
Within each unit, or patient, responses to therapy are likely to be correlated (eg, a single patient’s response to treatment A is correlated with that patient’s response to treatment B; the responses are not independent). This causes complexities in both the design and the analysis
Finally, if either of the therapy cures
the disease in toto (as an antibiotic for infectious disease) then,
naturally, no cross over can be done.




![Researchers evaluated the effectiveness of the cannabinoid dronabinol on central neuropathic pain in patients with multiple
sclerosis.[1] The effectiveness of cannabinoids in relieving pain caused by central lesions in multiple sclerosis had not been
investigated previously. A randomised double blind placebo controlled crossover trial study design was used. The
intervention was orally administered dronabinol at a maximum dose of 10 mg daily or corresponding placebo. Each treatment
period was for three weeks, separated by a three week washout period. All analgesic drugs, except for paracetamol, were
discontinued at least one week before the start of the trial.
The primary outcome was spontaneous pain intensity in the last week of each treatment period measured using a numerical
rating scale. The researchers reported that, when compared with placebo, dronabinol had a significant analgesic effect on central
pain in patients with multiple sclerosis. Although the effects were modest they were clinically relevant. The number of
patients with adverse events was higher during active treatment, especially in the first week of treatment. The functional ability
of the patients with regard to their multiple sclerosis did not change.
Which of the following statements, if any, are true?
a) All participants received both treatments in the same
sequence order
b) Each participant acted as his or her own control
c) The purpose of the washout period was to allow the effects
of the first treatment to dissipate before starting the second
treatment
d) The crossover study design required more participants
than if a “between subjects” study design had been used to
compare dronabinol and placebo](https://image.slidesharecdn.com/crossovertrial-250324055622-940f99e7/85/CROSS-OVER-TRIAL-EXPERIMENTAL-STUDY-DESIGN-63-320.jpg)



































































