Downloaded 14 times

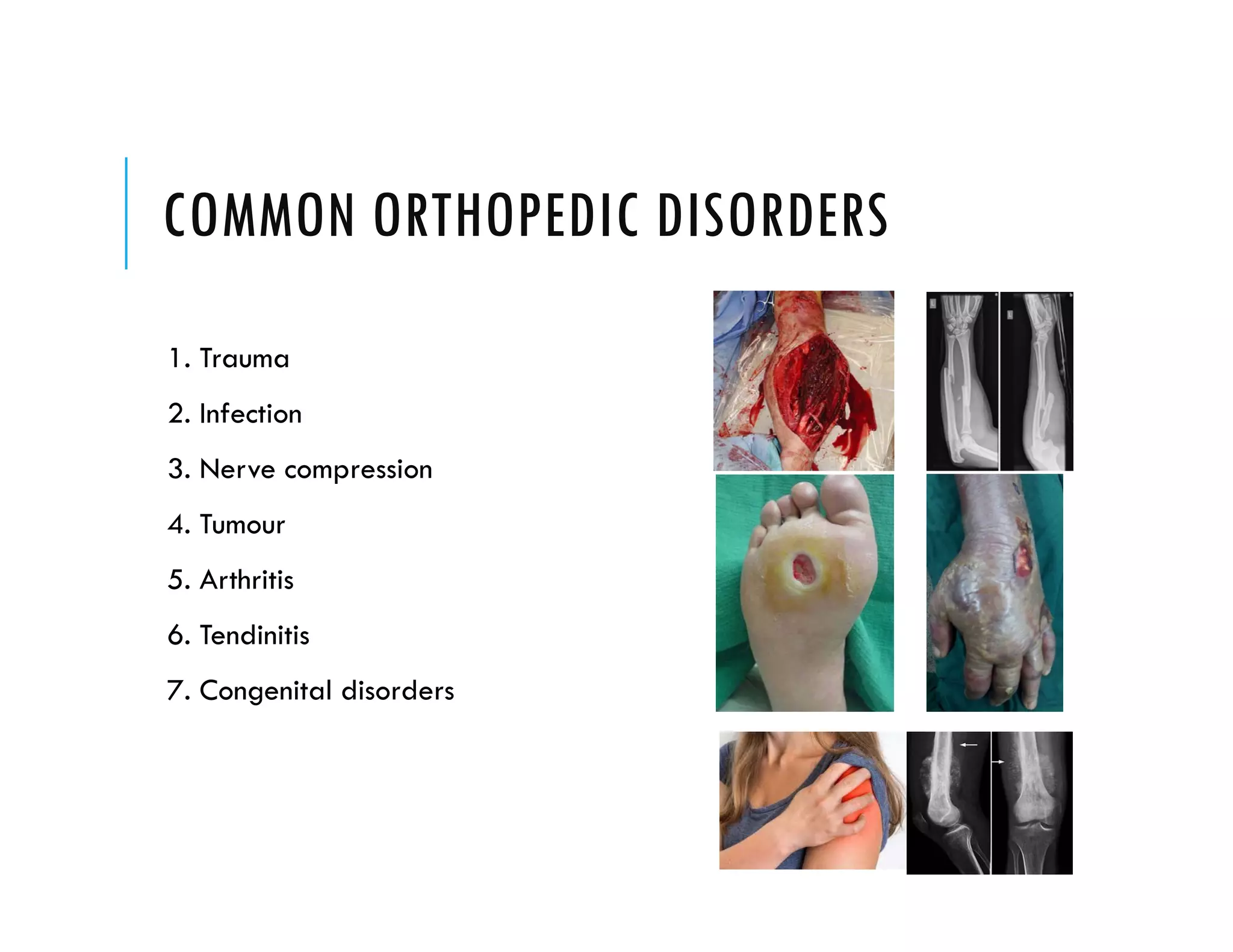






























































This document provides an overview of common orthopedic disorders including their causes, risk factors, symptoms, prevention strategies and treatment options. It discusses traumatic injuries like ankle sprains and wrist fractures. It also covers overuse injuries, infections, arthritis, nerve compression issues, congenital disorders, bone and soft tissue tumors, and tendon problems. Prevention focuses on lifestyle changes, proper equipment, exercises and early treatment when possible. Treatment varies from conservative options like rest, bracing and physical therapy to surgery when more serious.



































































