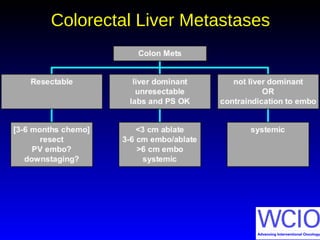
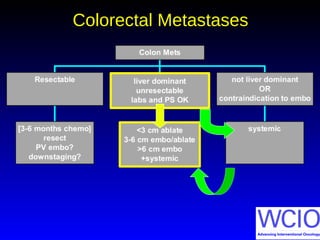
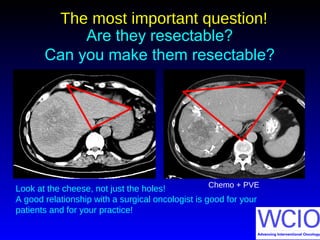
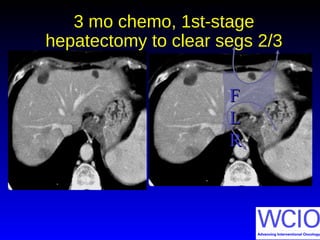
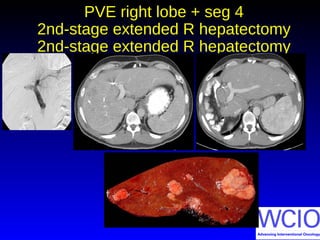
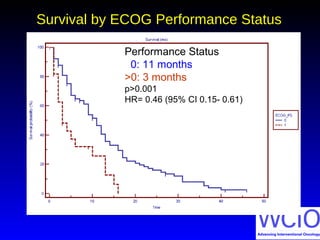
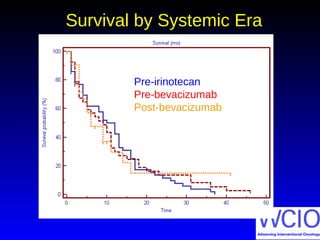
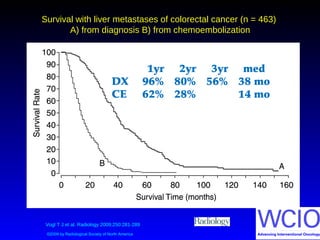
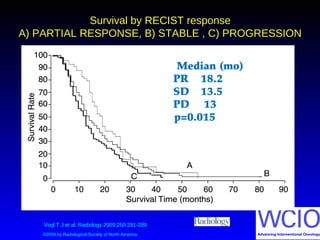
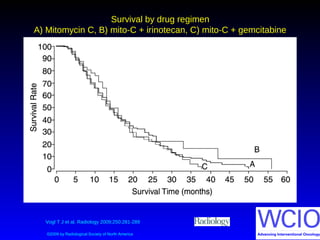
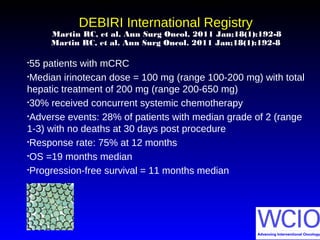
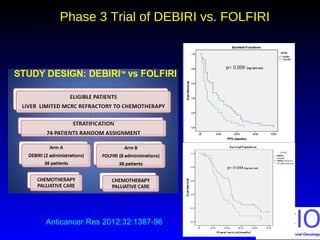
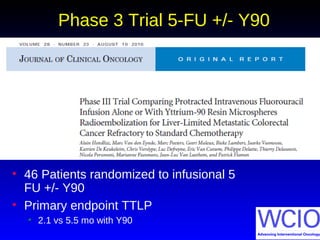
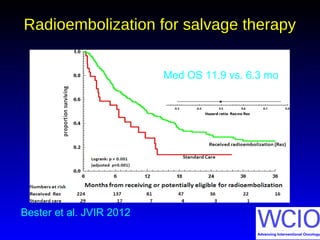
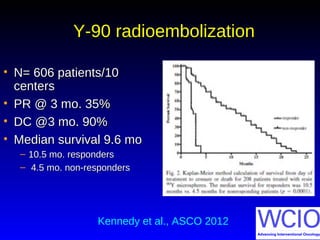
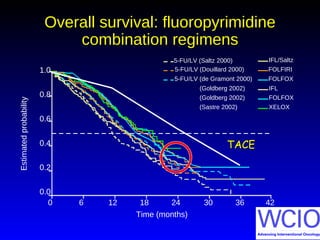
This document discusses treatment options for colorectal liver metastases, including systemic chemotherapy, surgical resection, chemoembolization, radioembolization, and portal vein embolization. It notes that systemic chemotherapy alone yields a median survival of 18-21 months but can downstage liver metastases to resectability in 20-25% of cases, resulting in a 5-year survival of 33%. Chemoembolization and radioembolization clinical trials demonstrate median survival ranges of 9-21 months. The document emphasizes the importance of the interventional oncologist in multidisciplinary care to increase the potential for curative resection through downstaging or portal vein embolization.
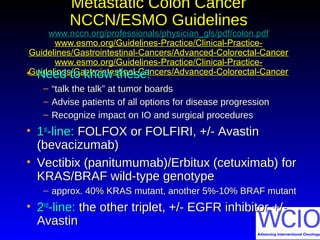
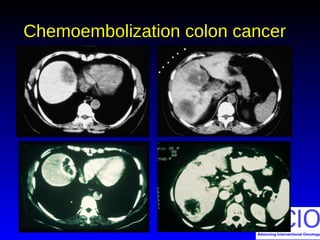
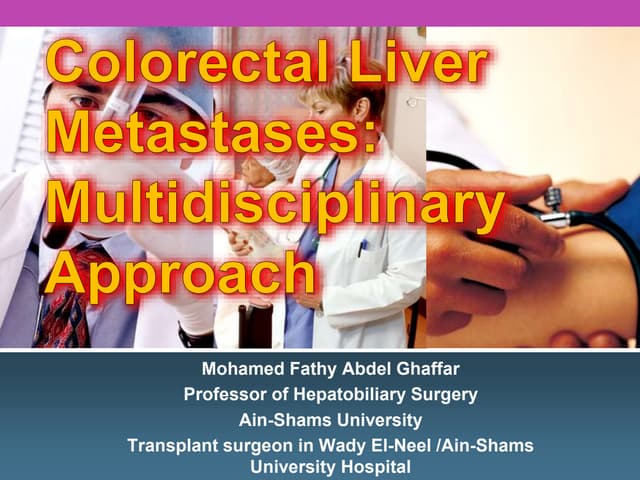
![Chemoembolization TrialsChemoembolization Trials
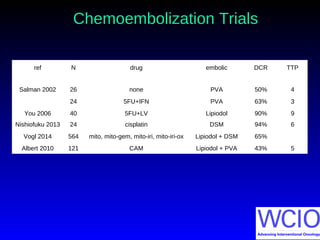
ref N median survival 1yr 2yr 3yr
from chemoembolization
Salman 2002 26 15 [8-17]
24 10 [8-11]
You 2006 40 16 90% 15%
Nishiofuku 2013 24 21 [8-24] 67% 42%
Vogl 2014 564 14.3 62% 28% 7%
Albert 2010 121 9 36% 13%
Hong 2009 21 7.7 43% 10%](https://image.slidesharecdn.com/13001320-michael-soulen-pairs-colon-2014-160212112306/85/COLON-CANCER-17-320.jpg)

























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









