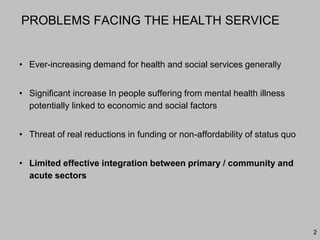

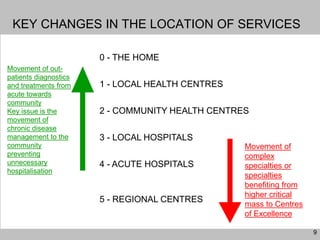
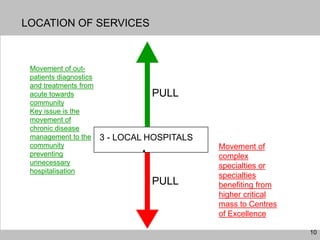
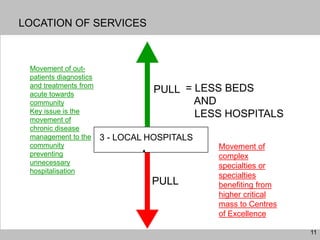
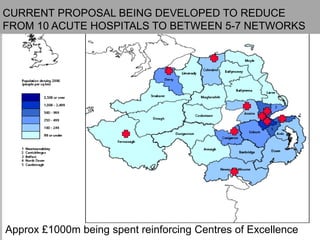
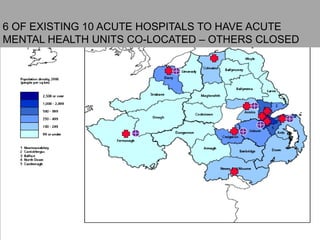
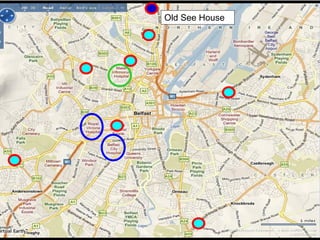





































































This document discusses plans to reduce acute mental health admissions in Northern Ireland by shifting services from hospitals to the community. It notes the growing costs and demand for health services that exceed available funding. The plan calls for integrating primary, community, and acute care through partnerships across sectors. Services will move from hospitals to health centers near patients' homes to allow earlier intervention, chronic disease management, and independent living with support. Acute mental health units will co-locate with hospitals but close standalone facilities, investing instead in community mental health teams and crisis services to prevent hospitalizations.






























































































