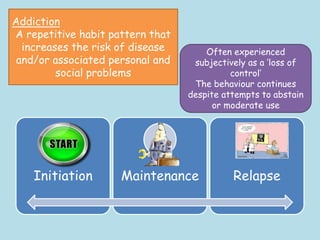
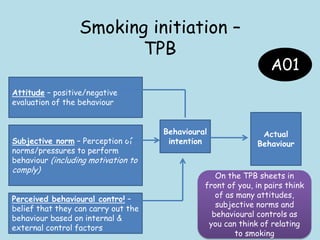
The document discusses biological, cognitive, and learning approaches to explaining addiction initiation, maintenance, and relapse. It focuses on applying these approaches to smoking and gambling addictions. Specifically, it discusses how the cognitive approach views addiction as stemming from dysfunctional beliefs and faulty thought processes. Addicts are seen as having impaired control over their actions due to cognitive biases and a preference for immediate rewards over future consequences. Various studies are described showing how cognitive factors like attitudes, norms, and intentions can predict smoking initiation in adolescents. The cognitive processing model also explains how addictive behaviors become automatic over time, maintaining the addiction. Cognitive biases are discussed as distorting rational decision making in gamblers and fueling relapse.