Download as PDF, PPTX
![When FDA Prior Review of a Study is Needed
• Drugs –
– it is illegal to introduce an unapproved drug (or an unlicensed
biologic) into commerce for a clinical study unless an
Investigational New Drug exemption (IND) is effective (or not
required)
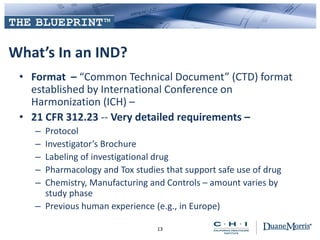
– IND regulations – 21 CFR Part 312
• Devices
– a device that otherwise would require an approved Premarket
Approval Application (PMA) or cleared premarket notification
[510(k)] can be shipped lawfully if to be studied in an
investigation to show safety or effectiveness if an Investigational
Device Exemption (IDE) is approved or the study is exempt
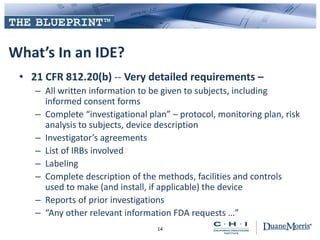
– IDE regulations – 21 CFR Part 812
6](https://image.slidesharecdn.com/chidmblueprint-swit-clinical-20130514-final-171125043933/85/Clinical-Trials-Regulatory-Privacy-Issues-6-320.jpg)
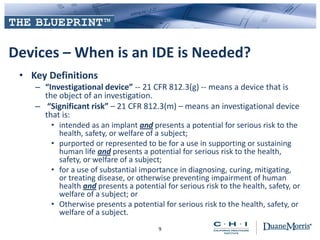
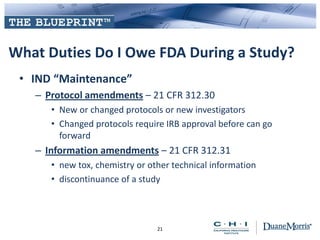
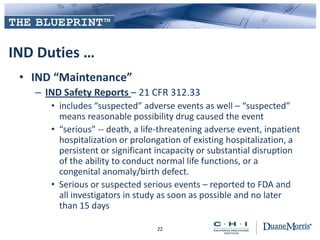
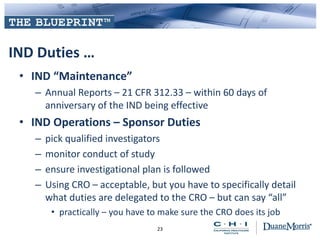
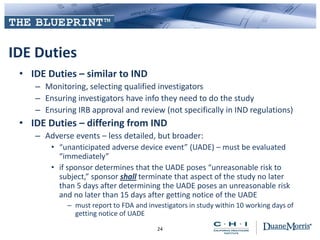
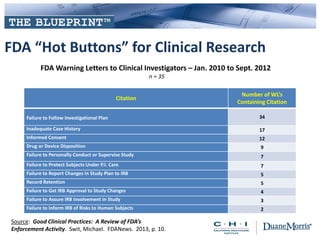
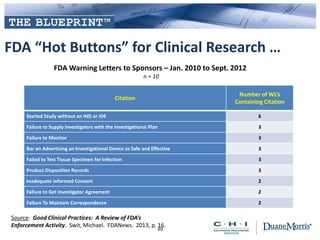



This document provides an overview of key regulatory and privacy issues related to clinical trials. It discusses the FDA requirements for clinical trials, including when an IND or IDE is needed prior to starting a study. It covers human subject protection duties around informed consent and IRB oversight. The document also outlines sponsor responsibilities during a study such as IND/IDE maintenance, safety reporting, and financial disclosure of clinical investigators. Finally, it discusses the role of HIPAA privacy rules and how protected health information can be used and disclosed for clinical research purposes.

















































































