Download to read offline



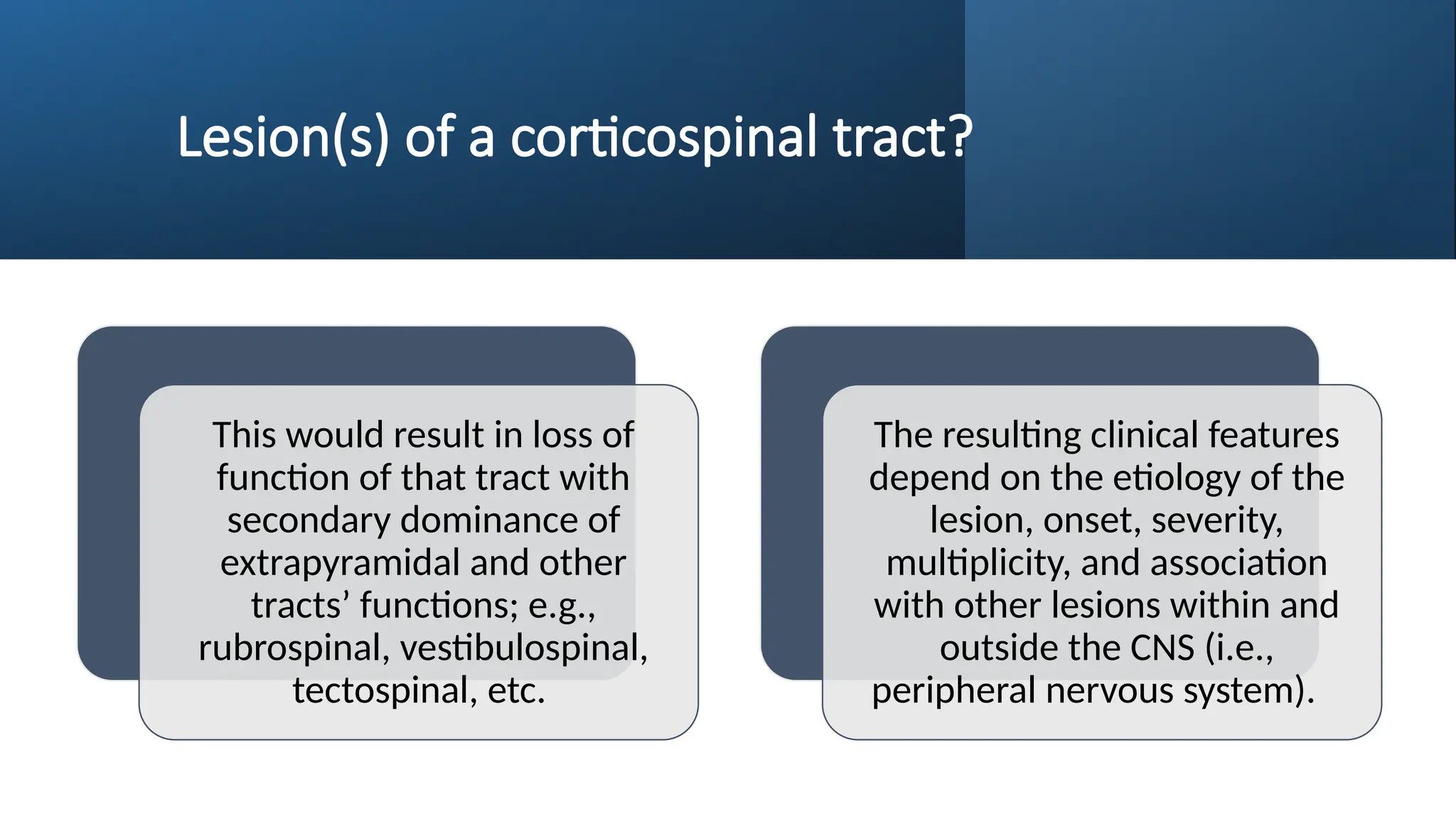
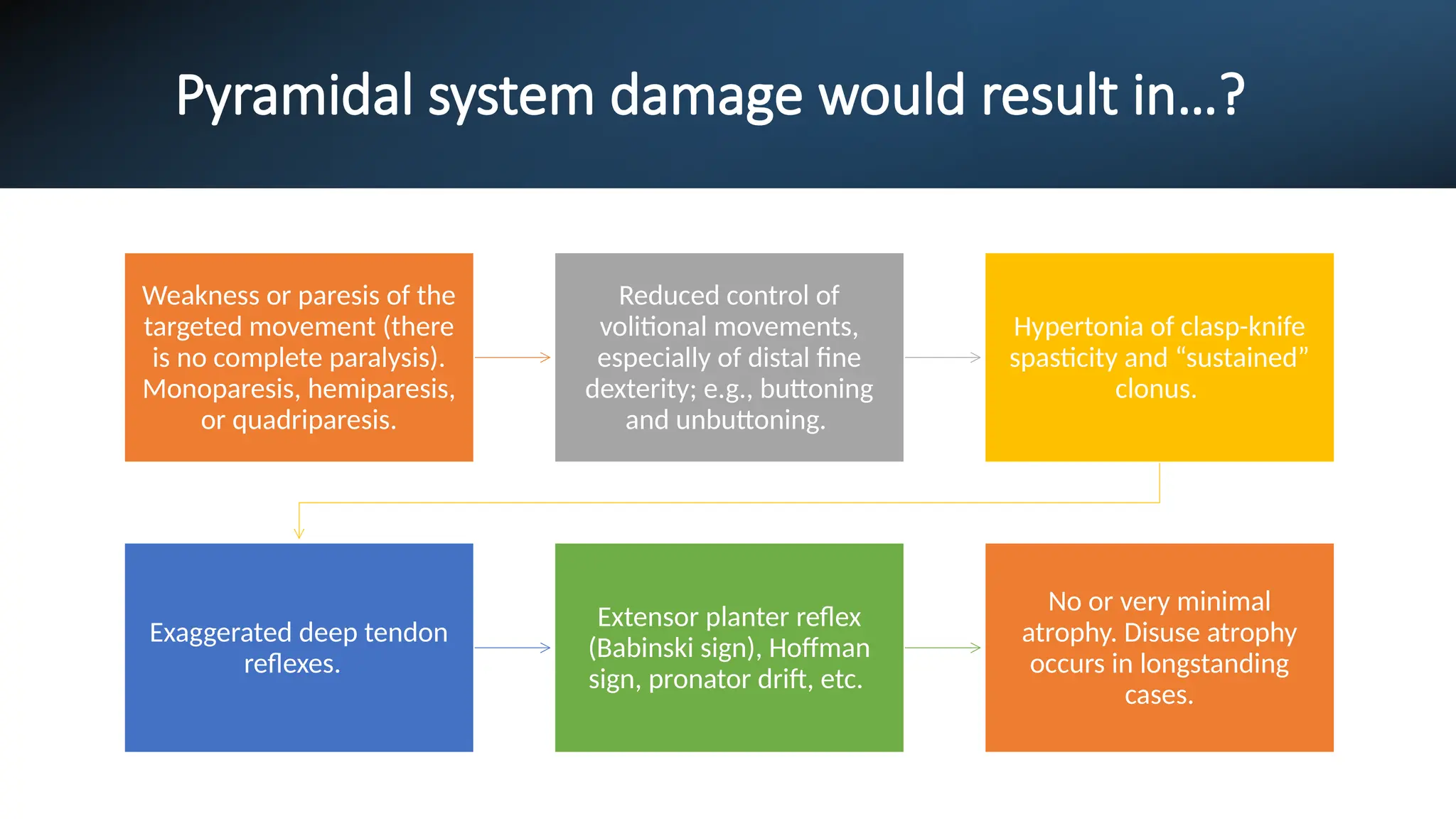





The document discusses the clinical aspects of upper and lower motor neuron lesions with a focus on the functions and disruptions of the corticospinal tracts. It describes the resulting symptoms from upper motor neuron lesions, such as weakness, hypertonia, and exaggerated reflexes, as well as the characteristics of lower motor neuron lesions, including weakness, hypotonia, and atrophy. The clinical presentation varies based on the etiology and location of the lesions.














![Central Nervstem notes [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/centralnervoussystemnotesautosaved-250325012003-ecd5223c-thumbnail.jpg?width=640&height=640&fit=bounds)













































