Download to read offline

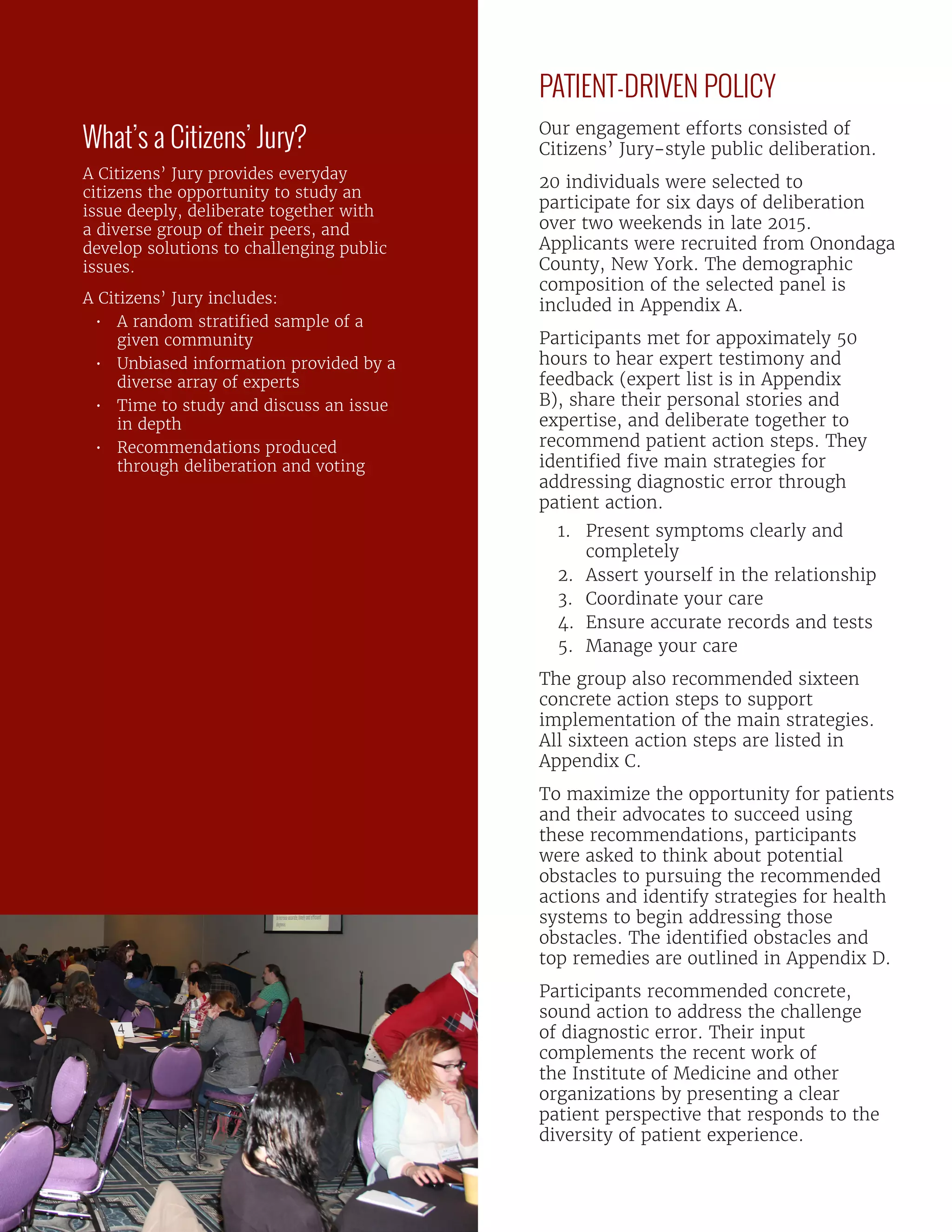
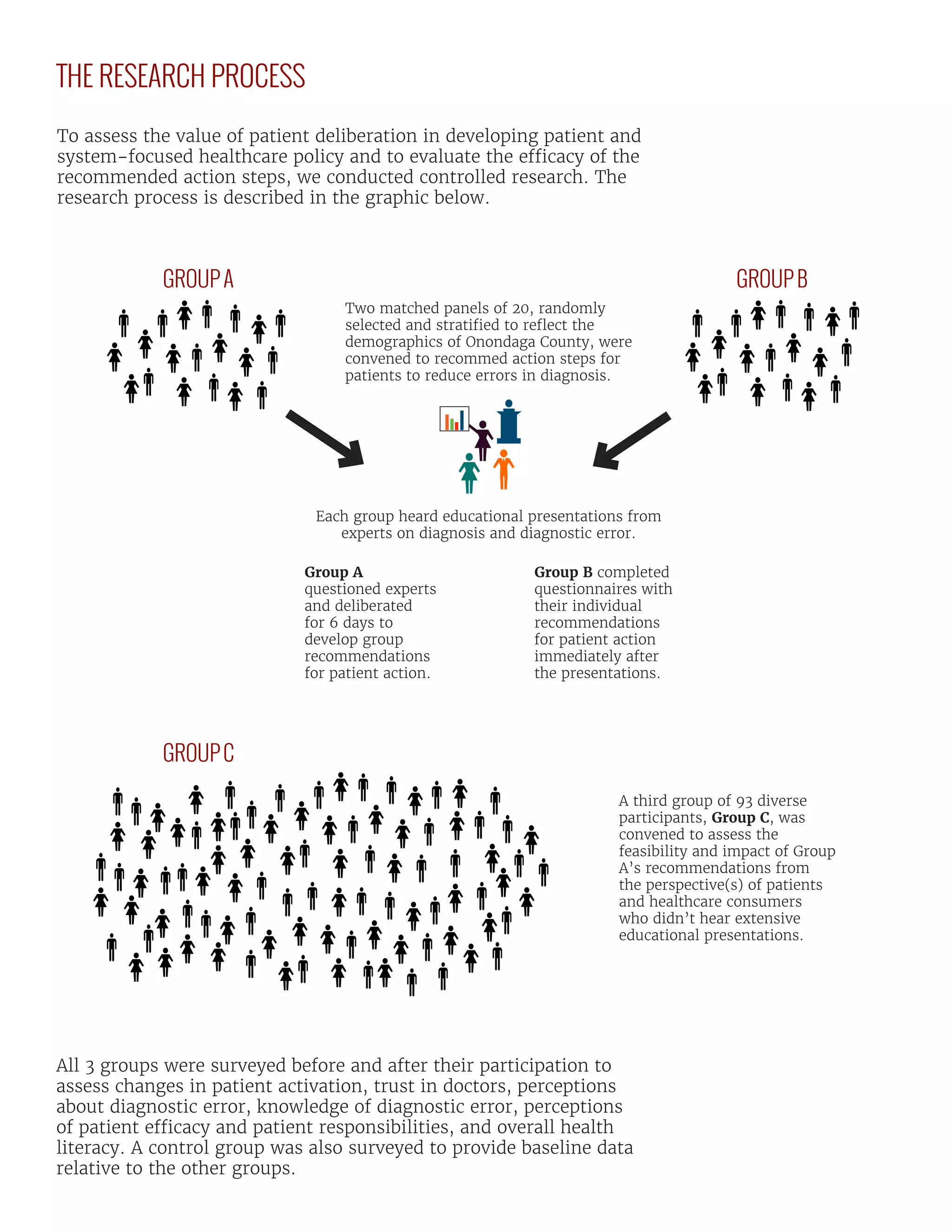
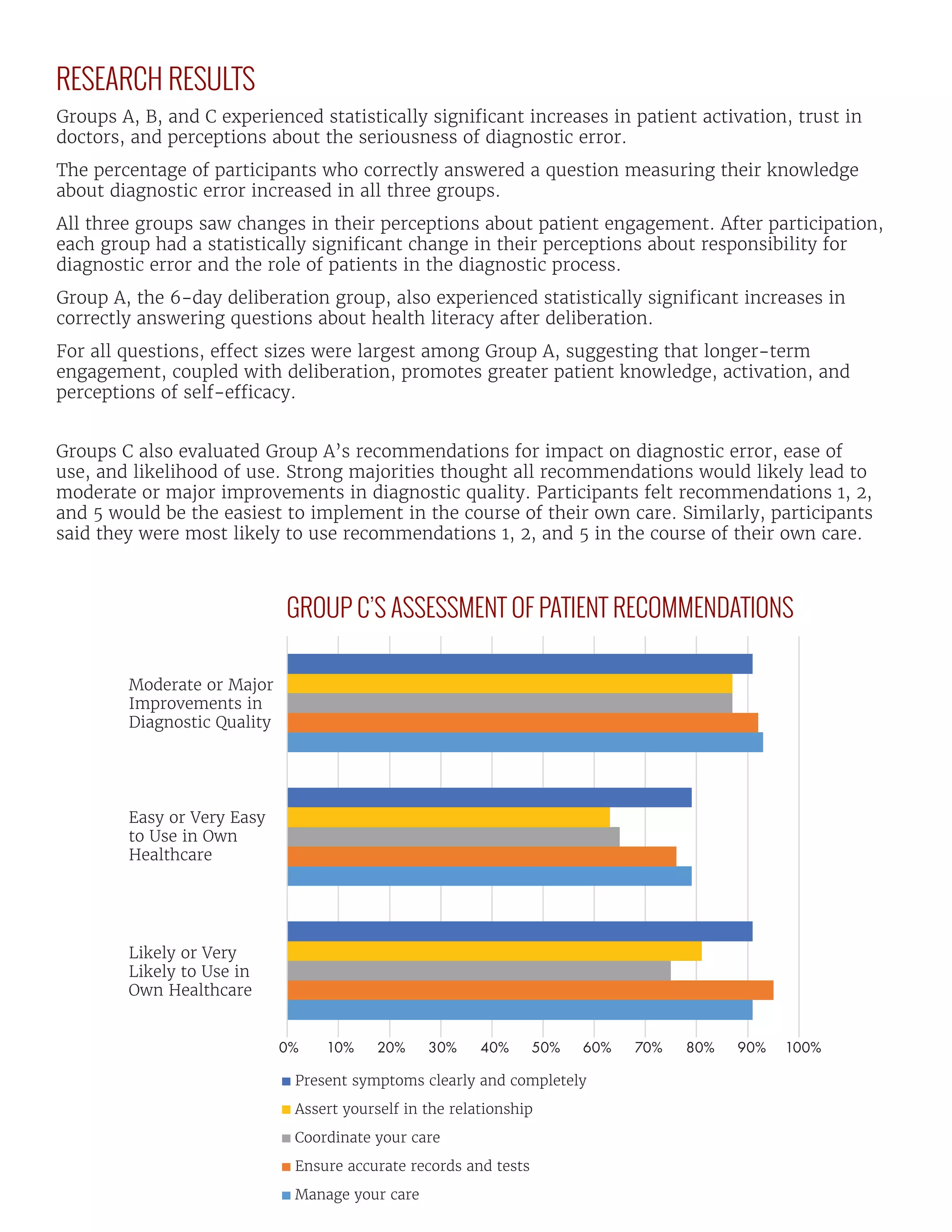


The Jefferson Center, in collaboration with Syracuse University and the Society to Improve Diagnosis in Medicine, is conducting a two-year initiative to assess public deliberation's value in healthcare policy, particularly in defining patient roles in improving diagnostic quality. By engaging diverse groups in public deliberation, they identify actionable strategies to address diagnostic errors and the obstacles patients face in the diagnostic process. The initiative’s findings emphasize the importance of patient involvement in healthcare, demonstrating that educated and activated patients can significantly enhance diagnosis and health outcomes.

![HIVProjectProgressPoster[1]](https://cdn.slidesharecdn.com/ss_thumbnails/d36eead9-2b43-4fa9-af11-0d2f69e3f49d-150421234017-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)













































































