1. UNDERSTANDING BARRIERS TO OBTAINING ORAL CANCER TREATMENT AND THEIR IMPACT
ON PATIENTS’ CANCER EXPERIENCE
Giovanna Braganza1, Taylor McEachon1, Kah Poh Loh1, Elizabeth Hansen1, Elizabeth Guancial1, Breton Roussel2, Derrick German1, Supriya G. Mohile1, Allison Magnuson1
1 University of Rochester James P. Wilmot Cancer Center, 2 Robert J. Wood School of Medicine at Rutgers University
The benefits of oral oncolytics include their ease of use,
convenience, and generally well-tolerated side effects when
compared to traditional intravenous chemotherapy. Although the cost
associated with oral oncolytic therapy is high and growing, research
into patient preferences and quality of life issues indicate that
patients prefer oral oncolytics over traditional intravenous
chemotherapy. Studies evaluating oral chemotherapy adherence
reveal an association between out of pocket expenses, social
support, treatment adherence, and outcomes. Currently there is
little data describing the psychosocial impact of the financial burden
associated with oral cancer medication and its influence on patient
satisfaction and medication adherence.
Through this study we hope to:
1. Assess the financial burden of obtaining oral cancer medication.
2. Measure out of pocket costs and psychosocial outcomes.
3. Observe associations between socioeconomic predictors and
financial toxicity.
4. Identify patient characteristics or other factors associated with
patterns of medication adherence.
Patients experienced significant costs associated with taking oral
oncolytic medications. Future work will assess satisfaction.
Increased cost sharing and wait time for delivery of medication may
be associated with higher psychosocial stress.
Future work should further evaluate factors associated with poor
medication adherence in patients taking oral cancer medications such
as memory, fatigue, and financial stress; future work will also evaluate
factors associated with poor adherence such as high symptom burden.
The study population comprised of patients 18 years and older with
solid tumor malignancy, excluding breast cancer, who were
prescribed an oral oncolytic at the University of Rochester Medical
Center. Study participants were followed from the time oral cancer
medication was prescribed until approximately 3 months after
receipt of medication. Validated patient reported outcomes tools and
interviews were utilized to measure the psychosocial impact of
prescription wait time and to quantify financial burden, document
side effect profile, and describe patient experience while taking
medication. Evaluation of medication adherence for patients with
genitourinary malignancy was measured through pill counts and a
comprehensive review of medication regiment at monthly intervals.
Methods
Objectives
Background
Conclusions
Results
Study Workflow
Assessment Tools
Survey Tools and Questionnaires
Baseline Survey
Demographics, Finances, Geriatric Depression Scale, Distress Scale,
OARS Medial Social Support, Comorbidity, Instrumental Activities of
Daily Living
Telephone
Survey
10-point worry scale regarding wait for oral cancer medication
Post Medication
Receipt Survey
Medication Adherence Questionnaire, finances, healthcare related
resources, NCNN Distress Management Survey, Press Gainey
Questionnaire, PRO-CTCAE
Follow-up
Survey
Medication Adherence Questionnaire, finances, healthcare related
resources, NCNN Distress Management Survey, Press Gainey
Questionnaire, PRO-CTCAE, CTSQ
Characteristics Frequency
Urologic Malignancy
N = 17
Non-Urologic Malignancy N= 21
Total Enrolled
N = 38
Average Age 62
Work Status
Employed 9
Unemployed 21
Healthcare Provider Subjects N = 20
Baseline Worry Scale 5.1 (0-10)
PMRS Worry Scale 4.3 (0-10)
Follow-Up Worry Scale 2.8 (0-10) 0
1
2
3
4
5
6
7
8
$0 -$199 $200 - $499 $500 - $999 $1000 - $4999 $5000 - $9999
Frequency
Monthly Out of Pocket Expense for Oral Oncolytics
Non- GU
GU
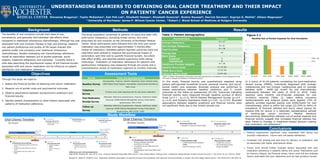
Table 1: Patient demographics
(Table 1) Patient demographic information was self-reported from the Baseline survey assessment tools
and used in analysis as predictors of financial toxicity.
Figure 1.1
In this study, financial toxicity was quantitatively assessed using
patient self-reported household income, personal income, and out-of-
pocket health care expenses. Bivariate analysis was performed to
assess associations between baseline predictors and 3- month
outcomes at the follow-up assessment (N=26). Outcomes indicating
financial toxicity were measured through baseline surveys of Worry
Scale (μ=5.1 , σX=3.3), NCCN Distress Management Survey (μ=3.9 ,
σX=2.4), and Geriatric Depression Scale (μ=3.03 , σX=2.53). Bivariate
associations between baseline predictors and financial toxicity were
not significant likely due to the limited sample size.
In a cohort of N=26 patients completing the post-medication
receipt survey (PMRS), individuals diagnosed with urologic
malignancies and non-urologic malignancies paid on average
between $299 - $499 per month for oral chemotherapy
medications between the years of 2014 to 2016. Costs
reported were monthly out-of-pocket expenses for oral
oncolytics received (Table 2), taken before insurance
reimbursements and external grants were applied. 23% of
patients enrolled reported paying over $500/month for oral
chemotherapy, which is within the range (22.55% to 64%) of
prevalence of financial distress and worry about paying for
medical bills for cancer in a nationally representative sample
of working-age cancer survivors.1 Medical literature
documenting relationships between out-of-pocket expense and
financial toxicity suggest that increased financial distress has
been linked to changes in treatment-related decision making
and medication non-adherence.2
References and Acknowledgements
Yabroff KR, Dowling EC, Guy GP Jr, et al.: Financial Hardship Associated With Cancer in the United States: Findings From a Population-Based Sample of Adult Cancer Survivors. J Clin Oncol 34 (3): 259-67, 2016.
Neugut AI, Subar M, Wilde ET, et al. Association between prescription co-payment amount and compliance with adjuvant hormonal therapy in women with early-stage breast cancer. J Clin Oncol.2011;29:2534–42