CIED POCKET INFECTION.pptx
•Download as PPTX, PDF•
0 likes•32 views

This document discusses cardiac implantable electronic device (CIED) pocket infections. It begins by defining CIED pocket infection and describing types such as early post-implantation inflammation and uncomplicated or complicated generator pocket infections. It then discusses the epidemiology, risk factors, microbiology, clinical features, evaluation and management approach, treatment including antibiotic therapy and device removal criteria, prevention strategies like antibiotic prophylaxis, and a study on the use of continuous targeted antibiotic delivery to treat pocket infections without device/lead extraction.

Recommended
Recommended
More Related Content
Similar to CIED POCKET INFECTION.pptx
Similar to CIED POCKET INFECTION.pptx (20)
Recently uploaded
Recently uploaded (20)
CIED POCKET INFECTION.pptx
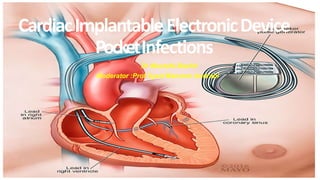
- 1. Cardiac Implantable Electronic Device PocketInfection Dr Mustafa Bashir Moderator :Prof Syed Manzoor Andrabi Implantable Cardiac Electronic Device Infection CardiacImplantableElectronicDevice PocketInfections Dr Mustafa Bashir Moderator :Prof Syed Manzoor Andrabi
- 2. CIED infections are generally considered in two categories: Pocket infection and systemic infection. An alternative approach to classification of CIED infection is by mode of infection : Primary infection occurs when the device and/or pocket itself is the source of infection; this is the most common form of CIED infection. Secondary infection occurs when the leads (and sometimes the device and the pocket) are seeded due to bacteremia from a remote source.
- 3. CIED pocket infection: CIED pocket infection refers to infection involving the subcutaneous pocket containing the pulse generator and the subcutaneous segment of the leads, but not the transvenous segment of the leads .
- 4. TYPES: Earlypost-implantation inflammation • Implantable Cardiac Electronic Device Infection Erythema affecting the implantation incision site, without purulent exudate, dehiscence, or systemic signs of infection and occurring within 30 days of implantation (stitch abcess) Uncomplicatedgeneratorpocketinfection • Purulent exudate (excluding simple stitch abscess), wound dehiscence, erosion through skin with exposure of the generator or leads, fluctuance (abscess) or fistula formation; AND no systemic symptoms or signs of infection AND negative blood cultures. Complicatedgeneratorpocketinfection • uncomplicated generator pocket infection WITH evidence of lead or endocardial involvement, systemic signs or symptoms of infection or positive blood cultures
- 5. Epidemiology Implantable Cardiac Electronic Device Infection • The overall incidence of ICED infections ranges from 0.5% to 2.2%. • Incidence of infection with primary implantation is 2- to 5-fold lower than for revision.
- 6. Risk factors: Host-related risks factors • End-stage kidney disease • Previous device infection • Corticosteroid use • Chronic obstructive lung disease • Malignancy • Diabetes mellitus • Heart failure • Anticoagulant use • Skin disorders • Older age with comorbidities • Pre-procedure fever Procedure-related risk factors • Procedure duration • Postoperative hematoma • Reintervention for lead dislodgement • Operator inexperience • Temporary pacing • Device replacement/revision • Lack of antibiotic prophylaxis Device-related characteristics: • Abdominal pocket • Positioning of two or more leads • ICD, CRT-P, or CRT-D greater risk than PPM
- 7. Microbiology: Hussein et al. J A C C : C L I N I C A L E L E C T R O P H Y S I OL OG Y V O L . 2 , NO . 4 , 2 0 1 6 Microbiology of CIED Infections A U G U S T 2 0 1 6 : 4 9 8 – 5 0 5 Implantable Cardiac Electronic Device Infection Staphylococcus aureus and coagulase-negative staphylococci (often Staphylococcus epidermidis) cause 65 to 75 percent of generator pocket infections and up to 89 percent of device- related endocarditis.
- 8. Implantable Cardiac Electronic Device Infection Clinicalfeatures: Patients with acute or subacute pocket infection may present with: pocket discomfort, Pocket deformity, erythema, swelling, and occasionally drainage through a dehisced incision.
- 10. Clinicalfeatures Implantable Cardiac Electronic Device Infection
- 12. Implantable Cardiac Electronic Device Infection
- 13. Approach to evaluation and management of suspected infection limited to cardiac implantable electronic device (CIED) pocket in adults
- 15. Management Recommendations Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint Working Party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society Implantable Cardiac Electronic Device Infection for Echocardiography (BSE). J Antimicrob Chemother 2015; 70 (2): 325-359. doi: 10.1093/jac/dku383
- 16. TREATMENT: Successful management of a CIED infection (systemic infection or pocket infection) requires: Antibiotic therapy Explantation of the entire CIED (leads, including residual leads that are nonfunctional, and pulse generator) Reimplantation of a new device (through an uninfected route), if indication for CIED persists.
- 17. Antibiotic therapy: Empiric antibiotic therapy for patients with suspected CIED infection should consist of antistaphylococcal therapy. Given the high incidence of methicillin-resistant Staphylococcus aureus (MRSA) and Staphylococcus epidermidis infection, initial therapy with vancomycin is reasonable. In patients presenting with hemodynamic instability, broadening of therapy to include gram-negative bacteria is appropriate (reasonable additions to vancomycin include piperacillin-tazobactam, cefepime,carbapenem, or gentamicin) High-dose daptomycin (8 to 10 mg/kg ideal body weight) is an acceptable alternative to vancomycin for treatment of device infection.
- 18. Device removal versus retention: Removal indications: TEE demonstrating valve or lead vegetation (as distinguished from noninfected fibrin stranding, which is often seen with long-duration leads). Blood cultures demonstrate: • Any isolation of the following organisms: S. aureus (especially in the absence of a clear portal of entry, occurring within three months of device manipulation, or persisting or recurring in spite of appropriate antimicrobial therapy) -Candida species • High-grade bacteremia (defined as two or more separate blood cultures positive for the same organism, drawn ≥1 hour apart)
- 19. Removal indications: Presence of pocket infection (based on clinical manifestations of pain or tenderness, erythema, swelling, purulent drainage, pocket deformation, adherence or threatened erosion, and/or percutaneous exposure/erosion of the generator and/or leads), with or without positive culture of pocket drainage or bacteremia.
- 20. Retention criteria : Device retention may be reasonably attempted in the following Circumstances: There is no clinical, TEE, or other imaging (if available) evidence of lead or valve Infection There is no evidence of pocket infection Bacteremia due to a pathogen other than S. aureus from a defined source other than the device or valvular infection.
- 21. Wilkoff, Bruce L., et al. "Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by t I h m e p A l a m n t e a r b i c l a e n C a H r e d a i a r t c A E s l e s c o t c r i o a n t i i o c n D ( e A v H i c A e ) I . n "fHeectaiortnrhythm6.7 (2009):1085-1104.
- 23. PREVENTION: Anticoagulation or antiplatelet therapy For patients with CHA DS –VASc <4 ) (eg, those not at high risk for embolic events), anticoagulation should be held prior to the procedure. Bridging anticoagulation with heparin is not recommended. Antiplatelet therapy should be held for 5 to 10 days before the procedure .
- 24. Antibiotic prophylaxis at device implantation Systemic antibiotic prophylaxis is warranted with antistaphylococcal antimicrobial drugs at the time CIEDs are implanted or generator units exchanged. The dosing regimens are cefazolin 2 g [3 g for those weighing >120 kg] intravenously within 60 minutes of surgical incision or, vancomycin 1 g intravenously within 90 to 120 minutes before the incision. For patients who cannot tolerate beta-lactam antibiotics or vancomycin, daptomycin or linezolid are alternatives • De Oliveira JC et al. Efficacy of antibiotic prophylaxis before the implantation of pacemakers and cardioverter defibrillators:results of a large, prospective, randomized, double-blinded,placebo-controlled trial. Circ Arrhythm Electrophysiol 2009; 2: 29–34.
- 25. Use of antibiotic-impregnated envelopes This approach is based on the reduction major CIED infections in certain higher-risk populations in the WRAP-IT trial . Absorbable mesh envelope that is impregnated with minocycline and rifampin is used.
- 26. Implantable Cardiac Electronic Device Infection Should temporary pacing be avoided to reduce infection? Recommendation:Wherever possible, temporary transvenous pacing should be avoided prior to implanting a permanent ICED. In a prospective multicenter survey of 6319 patients to determine complications occurring within 1 year of PPM or ICD implantation, the odds ratio of infection was 2.46 (95% CI 1.09–5.13) when a temporary wire was in situ. • Klug D, Balde M, Pavin D et al. Risk factors related to infections of implanted pacemakers and cardioverter-defibrillators: results of a large prospective study. Circulation 2007; 116: 1349–55.
- 29. OBJECTIVES: To evaluate the efficacy of delivering continuous, in situ–targeted, ultrahigh concentration of antibiotics (CITA) into the infected subcutaneous device pocket, obviating the need for device/lead extraction.
- 30. DESIGN: The CITA group consisted of 80 patients with pocket infection who were treated with CITA during 2007-2021. Of them, 9 patients declined lead extraction because of prohibitive operative risk, and 6 patients had questionable indications for extraction. Remaining 65 patients with pocket infection, who were eligible for extraction, but opted for CITA treatment, were compared with 81 patients with pocket infection and similar characteristics who underwent device/lead extraction as primary therapy
- 32. All the 80 patients included in the CITA cohort had definite, highly probable, or possible infection
- 33. Exclusion Patients with signs of systemic infection, fever, positive blood cultures or lead vegetations. Patients with Staphylococcus aureus growth in their CIED pocket cultures at the time of recruitment were excluded even in the absence of systemic infection. However, if S. aureus growth only appeared in cultures obtained during the surgical procedure performed as part of the already initiated CITA protocol, patients were allowed to continue participating in the study.
- 34. CITA procedure On admission, bacteriological cultures were obtained from secretions at dehisced wounds. A single intravenous dose of antibiotics (based on available bacterial information) was administered immediately after surgical specimens were sampled for culture. The wound edges of the CIED pocket and the fibrous capsule surrounding the device were conservatively debrided. Pocket cleansing entailed alternating 1.5% hydrogen peroxide and 5% povidone-iodine. A 6-F indwelling catheter was inserted percutaneously into the CIED pocket for antibiotic administration. The wound was covered by a sponge dressing and sealed with Negative-Pressure assisted Therapy for insulation
- 35. Device was continuously immersed in fluids containing ultrahigh concentrations of antibiotics. Loading dose of antibiotics delivered into the CIED pocket consisted of 1 to 2 g of vancomycin and/or 80 to 240 mg of gentamicin (or amikacin 250-500 mg), diluted in 25 to 50 mL of normal saline. Maintenance doses were delivered to the subcutaneous pocket continuously at 1 to 2 mL/h (40-80 mg/h of vancomycin and 3-10 mg/h of gentamycin). Patients with positive cultures received CITA for 14 days. Otherwise, CITA was discontinued at day 10.
- 36. Treatment of Pocket Infection With CITA 68-year-old man with an implanted cardiac resynchronization therapy device after 2 pocket revisions, the first for hematoma and the second for lead dislodgement, was referred to our center with pocket infection presenting as wound dehiscence and secretions growing Enterobacter cloacae (September 2019). (B) Minimally invasive surgery debridement of wound edges, thorough cleaning of the pocket, and eventual primary closure. (C) Wound sealed with sponge dressing and vacuum drainage during continuous inflow of ultrahigh concentrations of antibiotics (for 14 days). (D) The wound was closed primarily after removal of
- 37. Outcome measures: In the CITA cohort study ,the main outcome measure was the failure rate, defined as any of the following: 1) need for CIED/lead extraction or the development of chronic infection at any time; 2) death from any cause within 30 days postprocedure; or 3) death from infection related to the original pocket infection at any time during follow-up. In the case-control study of CITA vs CIED/lead extraction, the main outcomes included: 1) all-cause mortality (at 30 days and at 1 year) and 2) major complications (stroke, need for thoracotomy, urgent blood transfusions, or severe valvular damage) following extraction.
- 38. Results:
- 39. RESULTS: CITA was curative in 85% (n =68 of 80) of patients, who remained free of infection (median follow-up 3 years). In the case-control study of CITA vs device/lead extraction, cure rates were higher after device/lead extraction than after CITA (96.2% [n =78 of 81] vs 84.6% [n =55 of 65]. However, rates of serious complications were also higher after extraction (n =12 [14.8%] vs n =1 [1.5%]. All-cause 1-month and 1-year mortality were similar for CITA and device/lead extraction. Extraction was avoided in 90.8% (n ¼ 59 of 65) of extraction-eligible patients treated with CITA.
- 40. Limitations: S.-aureus infection, a pathogen notorious for its high virulence, were under-represented. Some patients categorized in the prohibitive-extraction subgroup could have been admitted to CIED/lead extraction programs in other centers. Also, complication rates from lead extraction are lower when performed in high volume specialized, referral centers.
- 41. THANK YOU Implantable Cardiac Electronic Device Infection T h a n k Y o u T H A THANK YOU