Hickman Catheter- An overview. Details about Hickman, insertion, care, maintenance, removal, complications.
•Download as PPTX, PDF•
0 likes•18 views

This is about different types of CVCs and especially about Hickman catheter, insertion, care and maintenance, complications and removal techniques.

Recommended
More Related Content
Similar to Hickman Catheter- An overview. Details about Hickman, insertion, care, maintenance, removal, complications.
Similar to Hickman Catheter- An overview. Details about Hickman, insertion, care, maintenance, removal, complications. (20)
More from Pritish Chandra Patra
More from Pritish Chandra Patra (14)
Recently uploaded
Recently uploaded (20)
Hickman Catheter- An overview. Details about Hickman, insertion, care, maintenance, removal, complications.
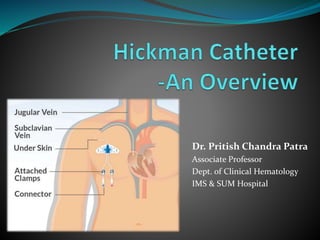
- 1. Dr. Pritish Chandra Patra Associate Professor Dept. of Clinical Hematology IMS & SUM Hospital
- 2. History Werner Forssmann Davies MK, Hollman A. Werner Forssmann. Heart. 2002 May;87(5):409. PMCID: PMC1767093
- 3. Landmarks 1 1929 1956 1950 “Forssmann” described the advance of a ureteral catheter to the heart by puncturing his own arm vein “Aubaniac” reported about the puncture of the subclavian vein Got Nobel prize This puncture technique helped to broaden the use of this technically demanding procedure
- 4. Introduction Central venous access is a commonly performed procedure with approximately 8% of hospitalised patients during their hospital stay.
- 5. Indications Quick administration of large volume of fluids or drugs Administration of i.v. fluids or drugs in the event of the collapse of peripheral vessels (shock) Administration of irritant or toxic drugs Administration of high-osmolarity solutions, e.g. TPN Longer therapies- lasting several days or weeks which require a venous access Dialysis Measurement of CVP
- 6. Types Non-Tunneled CVC Tunneled CVC Implanted Port PICC
- 7. Non-tunneled CVC Placed percutaneously Catheter exits the skin in the vicinity of the venous cannulation site Most commonly used for temporary access to the central circulation Lengths 15- 30 cm Materials polyurethane, silicone Valved catheters limit backflow of blood prevent infection & catheter thrombosis
- 8. Non-tunneled CVC Lumen- 1/2/3/4/… The distal hole is more reliable for drawing blood - doesn’t get suctioned against the wall of the vein during aspiration. ↑ number of lumen >> ↑ overall diameter of the catheter >> ↓ diameter of the individual lumen ↑ no of lumens >> ↓ maximum infusion rate >> ↑ rate of catheter thrombosis
- 9. Tunneled CVC Robert O. Hickman A pediatric nephrologist and inventor of a catheter that revolutionized care for patients with cancer, died on April 4, 2019. He was 92. In 1970, he was a founding member of the transplant team at Fred Hutchinson Cancer Research Center (Fred Hutch), Seattle that pioneered the BMT procedure.
- 10. Tunneled CVC- Hickman Traverses a subcutaneous tunnel between the catheterized vein and the skin exit site. Internal Jugular Vein
- 11. Tunneled CVC Hickman Round Material: Silicone Tip: soft and atraumatic Lumen- 1/2/3 Sizes- 4.2 to 12 F (Hickman, Broviac, Leonard) A cuff (Velour, Dacron) in the subcutaneous tissue adjacent the exit site Inflammatory response Allows fibroblastic ingrowth Prevents ascending infection Fixation- 3-4 weeks Rates of infection - lower than those of non-tunneled CVCs cuff
- 12. Tunneled CVC C-arm- for guidance and to confirm the tip position Anesthesia Adult- LA Children- GA Suture temporary Dacron cuff seals it later Loop catheter under sterile dressing- tension reliving loop
- 16. Tunneled CVC- advantages LONGER STAY LESSER MAINTENANCE LESSER INFECTIONS
- 17. Contra-indications Patient is allergic to the CVC material Past irradiation to the insertion site Previous episode of venous thrombosis at the site Previous history of vascular surgery at the site Avoid placement under the arm in the breast In soft tissue of the abdomen
- 18. Other CVCs- Implanted Ports
- 19. Other CVCs- PICC lines
- 20. Antibiotic prophylaxis CDC, USA (O’Grady et al., 2002)- use of antimicrobial prophylaxis routinely before insertion or during use of an intravascular catheter does not prevent catheter colonization or BSI
- 21. Catheter insertion Only experienced personnel should insert central venous catheters to minimize infection and other complications particularly in the presence of low platelets deranged clotting profile in critically ill patients
- 22. Catheter insertion Procedure should be performed in a clean area designated for CVC insertion such as OT or a procedure suite where high standard of asepsis is practiced. Risk of infection depends mainly on the presence of bacteria on the skin. Skin cleansing is the most important part of care before catheter insertion.
- 23. Cleansing Povidone iodine 2% aqueous chlorhexidine 2% chlorhexidine in alcohol
- 24. Long term care- Flushing Heparin Vs Normal Saline Exposure to heparin should be minimized to prevent HIT to avoid bleeding complications Prevent rupture smaller syringes create greater pressure Use 10ml syringes ONLY Prevent back flow pulsatile flush method– push–pause-push–pause maintain +ve pressure while removing the syringe Passannante & Macik, 1998 Pellowe et al. 2004 Conn, 1993; Primhak, 1998 Goodwin & Carlson, 1993; Dougherty, 2004
- 25. Long term care Patient education Hand washing Chlorhexidine gluconate Sterile gloves or clean gloves
- 26. Complications The main complications are- catheter-related infection catheter malfunction catheter-related thrombosis
- 27. Catheter-related infections Infection rates vary from 0.08 per 1000 days in oncology outpatients to 19/1000 catheter days in the critically ill. Hemato-oncology infection rates probably lie somewhere within this range. CRBSI can be severe and life-threatening depending on the micro-organism involved. Fletcher, 2005
- 28. Catheter-related infections CRBSI (catheter-related blood stream infection) ≥2 blood cultures +ve with the same organism from ≥2 separate sites at different times, in association with e/o colonization with the same organism Exit site infection Erythema Tenderness Discharge Tunnel infection Pain Induration along the track of the catheter
- 29. Category Non-neutropenic patient Neutropenic patient Exit site infection •Remove catheter if no longer needed •Treat empirically with *flucloxacillin •Remove catheter if no longer needed •Initial empirical therapy including glycopeptide •Treat for 10–14 days or longer until infection resolved •Modify according to isolates •Remove catheter •if evidence of progression or •if blood cultures are positive for Staph. aureus, Pseudomonas spp., Mycobacterium spp., or fungi Tunnel infection •Remove catheter if no longer needed •Treat empirically with *flucloxacillin •Remove catheter if no longer needed •Initial empirical therapy including glycopeptide •Treat for 10–14 days or longer until resolution of soft tissue infection. Modify according to isolates •If tracking continues to spread remove catheter Presumed CRBSI •Remove catheter if no longer needed •Treat empirically with antibiotics targeted against isolates •Remove catheter if no longer needed •Initial empirical antibiotic therapy. Modify according to isolates. •Treat for at least 10–14 days •Remove catheter •if cultures remain positive after 48 h of therapy or •if proven catheter-related infection with Staph. Aureus, Pseudomonas spp., Mycobacterium spp., or fungi *Unless known to be colonized with MRSA, when a glycopeptide should be used
- 30. ‘Antibiotic lock’ technique May be effective in reducing catheter-related bacteremia A technique by which an antimicrobial solution is used to fill a catheter lumen allowed to dwell for a period of time while the catheter is idle
- 31. Antibiotics- vancomycin, gentamicin, ciprofloxacin, minocycline, amikacin, cefazolin, cefotaxime, and ceftazidime Antiseptics- taurolidine, trisodium citrate Anticoagulant- heparin or EDTA Designed to render the internal flow passages resistant to clot formation and hostile to bacterial and fungal growth. There are no FDA approved formulations. ‘Antibiotic lock’ technique
- 32. Catheter removal Indications catheter related infection Staph. aureus, Pseudomonas spp., Mycobacterium spp., or fungi persistent catheter occlusion catheter-related thrombus damaged catheter end of treatment
- 33. Removing the Hickman catheter Removed by surgeon Pinch off Catheter breakage Catheter embolism
- 34. Catheter removal Local anesthetic and minor surgical cut-down to remove the cuff Remove the catheter in the direction of the tunnel Catheter should be inspected carefully after removal to ensure that it is complete If infection is suspected, send tip for culture The cutdown site should be sutured with a fine 3/0 or 4/0 monofilament suture After removal, apply pressure to the exit point, tunnel and an occlusive dressing placed over the exit site to avoid air embolism.
- 35. Indian experience of CVCs
- 36. A total of 213 CVCs were inserted in patients with hematological (62%) and solid organ malignancies (38%). Ninety-eight patients (46%) had peripheral inserted central catheter (PICC), 90 (42%) patients had Hickman catheters and 25 (12%) had a port. The median duration of retention of Hickman catheters was 104 days (3-365 days), for the peripherally inserted central catheters was 59 days (3-100 days) and for the port it was 280 days (45-365 days). Non-infective complications were more than infective (12% vs. 7%). The most common complication was non-infective occlusion and thrombophlebitis. In one patient with PICC thrombosis occurred in the cephalic, radial and ulnar vein and in one patient with port thrombosis occurred in the superior vena cava. Organisms were isolated in 60% (12 out of 20) of cultures. Common organisms isolated were Pseudomonas aeruginosa in 5 (42%), Staphylococcus aureus in 2 (16%), Escherichia coli in 2 (16%) and Aspergillus in 3 (25%) patients. 7 out of 12 infected patients had negative blood cultures within 7 days of antibiotic treatment, 5 patients remained positive for more than 7 days with antibiotics. In 155 patients (73%), the desired treatment protocol was completed and at present there are still 28 patients (13%) with catheters. 5 patients (2.3%) died of febrile neutropenia and septicemia with multi-organ failure. In 5 patients (2.3%), the catheters (1 Port, 1 Hickman and 3 PICC) were prematurely removed because of thrombosis.
- 37. A total of 111 catheters were used in 110 patients. Two catheters were used in one patient due to loss of first catheter due to rupture. Duration of catheter indwelling period ranged from 7 to 365 days with a median of 120 days. In 99 out of 111 (90%) cases catheter tip was located either in superior vena cava or in right atrium. Total catheter related complications occurred in 37 (34.5%) patients and total catheter loss due to complications were documented in 17 (15.4%) patients. A total of 8 catheters (7.27%) were lost due to infective complications. Two-thirds of these cases had infection during the granulocytopenic phase of chemotherapy (TLC < 1000/dl). Exit site infection, catheter blood culture proven bacteraemia and PUO were seen in 3, 6, and 10 patients respectively. All 3 exit site infections were treated with local dressing and antibiotics. Seven out of 10 PUO and 1 out of 6 systemic bacteraemias were managed by giving systemic antibiotics. Five patients with blood culture proven bacteraemia and 3 patients with PUO did not respond to systemic antibiotics necessiating catheter removal. Staphylococcus aureus was found in 4 and candida albicans in 2 patients in blood culture proven bacteraemia cases while Staphylococcus aureus was found in 3 patients of PUO. A total of 9 catheters were lost due to non-infective complication. Seven (6.36%) catheters were lost due to blockage and, 1 catheter was lost due to extrusion and one due to rupture during infusion. Blockage of catheter occurred in 16 patients out of which 9 could be salvaged by flushing with heparin saline. One patient had supraventricular tachycardia during the insertion of the catheter which returned to normal sinus rhythm promptly on withdrawing the catheter. We did not encounter any haemorrhagic complications.
- 38. Summary In high-risk cancer patients it may not be possible to prevent nosocomial infections. However, with appropriate use of CVAD devices and careful infection control measures, these devices may help to facilitate care without added risk of infection.
- 39. References Guidelines on the insertion and management of central venous access devices in adults L. BISHOP*, L. DOUGHERTY†, A. BODENHAM‡, J. MANSI*, P. ROWE§, C. KIBBLER–, M. SHANNON**, J. RELEAVEN†:6 February 2007 CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011 Experience with Venous Access Devices in Pediatric Cancer Patients, Tulika seth, INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 25 No. 2, 2004 A retrospective study of central venous catheters GCRI experience Sachin A. Jain etal, Indian J Med Paediatr Oncol. 2013 Oct-Dec; 34(4): 238–241. An analysis of long-term venous access catheters in cancer patients:experience from a tertiary care centre in India. NK Shukla, DK Das, SV Deo, V Raina
- 40. Thank You
Editor's Notes
- Dacron is a registered trade name for a polyester fiber made by DuPont. Dacron is especially known for its durability, consistency, and quality. Dacron, unlike natural fibers, is hypoallergenic, non-absorbent, and mildew-resistant. Velour is made from polyester, spandex, or cotton, or a cotton-polyester blend.