Downloaded 19 times


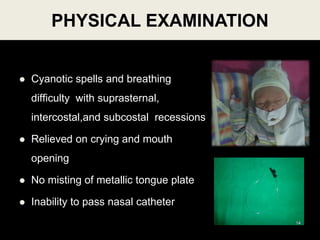
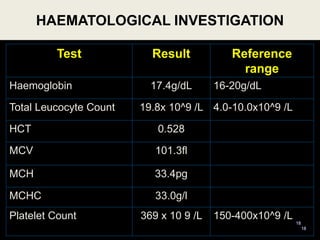
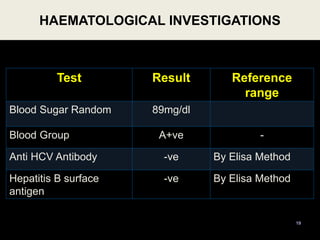

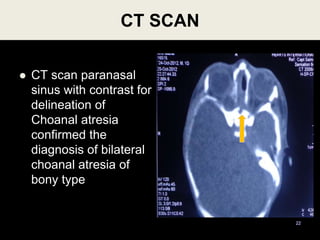
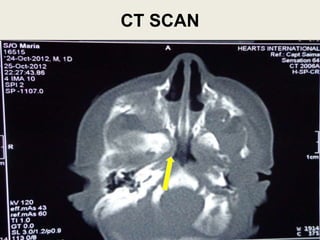
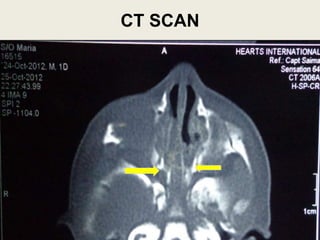
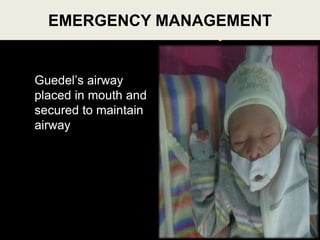
















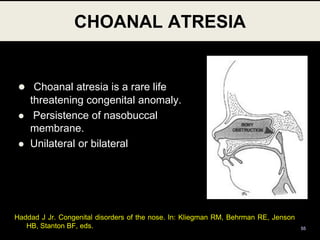
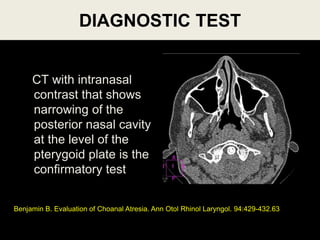
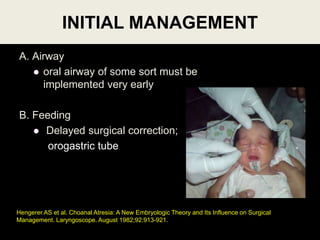


The document discusses the case of a newborn male patient presenting with breathing difficulty and cyanotic spells since birth. Examination revealed bilateral choanal atresia, which was confirmed by CT scan. The patient underwent transnasal endoscopic surgery to repair the atresia. Post-operatively he was cared for in the neonatal ICU and recovered well. The document also provides background information on choanal atresia including epidemiology, etiology, pathogenesis, clinical presentation, diagnosis, management including surgical techniques, and post-operative care.






























































































