Download to read offline

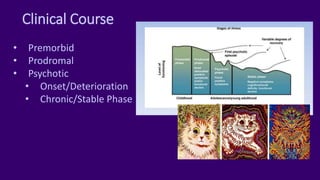

This document provides an overview of schizophrenia, detailing its diagnosis, symptoms, subtypes, and treatment options. It discusses criteria from the DSM-5 and explores various causative theories related to genetics, environment, and neurobiology. Additionally, it highlights the clinical course of the disorder and includes references for further reading.












































































