Downloaded 129 times
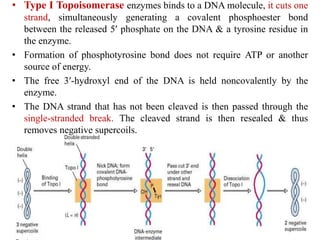
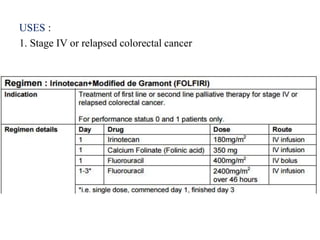
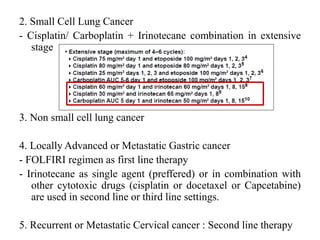
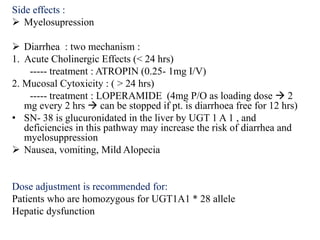
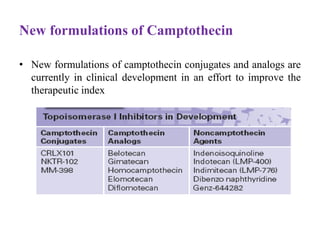
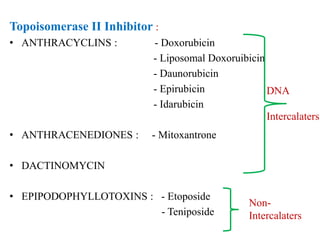
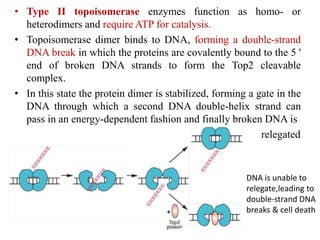
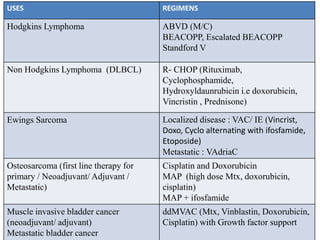
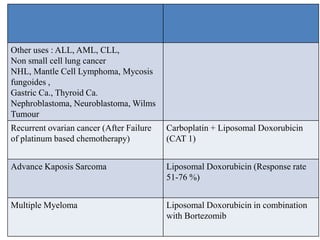

Topoisomerases are enzymes that regulate DNA topology during replication and transcription by introducing temporary breaks in DNA strands. Topoisomerase inhibitors can be classified as topoisomerase I or II inhibitors. Camptothecins like irinotecan and topotecan are topoisomerase I inhibitors that stabilize the covalent complex between topoisomerase I and DNA, preventing rejoining of DNA strands. They are used to treat colorectal cancer and other cancers. Anthracyclines like doxorubicin are topoisomerase II inhibitors that stabilize cleavable complexes and cause DNA damage. They are commonly used to treat breast cancer, lymphomas, sarcomas and other cancers. Both classes
















































![Chapter 39 role of radiotherapy in benign diseases.pptx [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter39roleofradiotherapyinbenigndiseases-191105205437-thumbnail.jpg?width=640&height=640&fit=bounds)






































