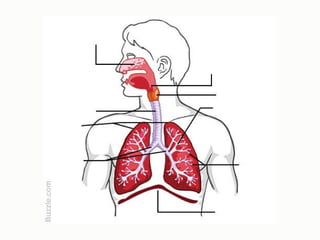
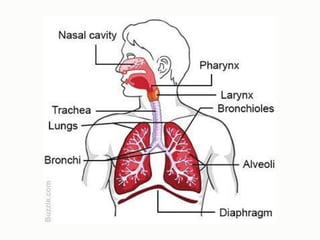
Organs of theRespiratory System
• Nasal cavity/ Nose
• Pharynx
• Larynx
• Trachea
• Lungs
• Bronchi
• Alveoli
• Diaphragm
5.
Functional Anatomy ofthe Respiratory
System
• Gas exchanges between the blood and external
environment occur only in the alveoli of the lungs
• Upper respiratory tract includes passageways
from the nose to larynx
• Lower respiratory tract includes passageways
from trachea to alveoli
⚬Passageways to the lungs purify, humidify, and warm
the incoming air
6.
The Nose
• Theonly externally visible part of the respiratory
system
⚬Nostrils (nares) are the route through which air enters
the nose
⚬Nasal cavity is the interior of the nose
⚬Nasal septum divides the nasal cavity
7.
Frontal sinus
Oropharynx
Trachea
Nasal cavity
Hyoidbone
Cribriform plate
of ethmoid bone
• Palatine
tonsil
• Lingual
tonsil
Laryngopharynx
Esophagus
• Nasal conchae (superior,
middle, and inferior)
• Nasal meatuses (superior,
middle, and inferior)
• Nasal
vestibule
• Nostril
Hard palate
Soft palate
Tongue
Larynx
• Epiglottis
• Thyroid cartilage
• Vocal fold
• Cricoid cartilage
Sphenoidal sinus
Posterior nasal
aperture
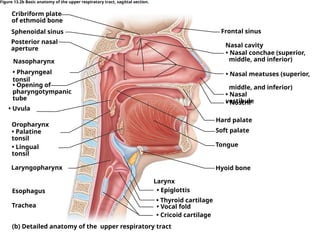
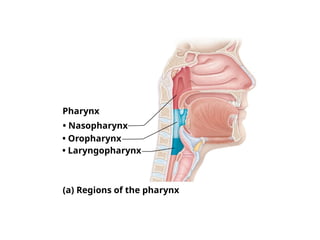
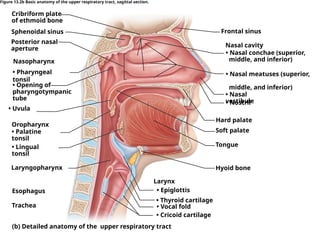
Figure 13.2b Basic anatomy of the upper respiratory tract, sagittal section.
(b) Detailed anatomy of the upper respiratory tract
• Opening of
pharyngotympanic
tube
Nasopharynx
• Pharyngeal
tonsil
• Uvula
8.
The Nose
• Olfactoryreceptors are located in the mucosa on
the superior surface
• The rest of the cavity is lined with respiratory
mucosa, which
⚬Moistens air
⚬Traps incoming foreign particles
⚬Enzymes in the mucus destroy bacteria chemically
9.
The Nose
• Conchaeare projections from the lateral walls
⚬Increase surface area
⚬Increase air turbulence within the nasal cavity
⚬Increased trapping of inhaled particles
• The palate separates the nasal cavity from the
oral cavity
⚬Hard palate is anterior and supported by bone
⚬Soft palate is posterior and unsupported
10.
The Nose
• Paranasalsinuses
⚬Cavities within the frontal, sphenoid, ethmoid, and
maxillary bones surrounding the nasal cavity
⚬Sinuses:
■ Lighten the skull
■ Act as resonance chambers for speech
■ Produce mucus
11.
The Pharynx
• Commonlycalled the throat
• Muscular passageway from nasal cavity to larynx
⚬Continuous with the posterior nasal aperture
• Three regions of the pharynx
1.Nasopharynx—superior region behind nasal cavity
2.Oropharynx—middle region behind mouth
3.Laryngopharynx—inferior region attached to larynx
12.
The Pharynx
• Oropharynxand laryngopharynx serve as
common passageway for air and food
⚬Epiglottis routes food into the posterior tube, the
esophagus
• Pharyngotympanic tubes open into the
nasopharynx
⚬Drain the middle ear
The Pharynx
• Tonsilsare clusters of lymphatic tissue that play a
role in protecting the body from infection
⚬Pharyngeal tonsil (adenoid), a single tonsil, is located in
the nasopharynx
⚬Palatine tonsils (2) are located in the oropharynx at the
end of the soft palate
⚬Lingual tonsils (2) are found at the base of the tongue
15.
Frontal sinus
Oropharynx
Trachea
Nasal cavity
Hyoidbone
Cribriform plate
of ethmoid bone
• Palatine
tonsil
• Lingual
tonsil
Laryngopharynx
Esophagus
• Nasal conchae (superior,
middle, and inferior)
• Nasal meatuses (superior,
middle, and inferior)
• Nasal
vestibule
• Nostril
Hard palate
Soft palate
Tongue
Larynx
• Epiglottis
• Thyroid cartilage
• Vocal fold
• Cricoid cartilage
Sphenoidal sinus
Posterior nasal
aperture
Figure 13.2b Basic anatomy of the upper respiratory tract, sagittal section.
(b) Detailed anatomy of the upper respiratory tract
• Opening of
pharyngotympanic
tube
Nasopharynx
• Pharyngeal
tonsil
• Uvula
16.
The Larynx
• Commonlycalled the voice box
• Functions
⚬Routes air and food into proper channels
⚬Plays a role in speech
• Located inferior to the pharynx
• Made of eight rigid hyaline cartilages
⚬Thyroid cartilage (Adam’s apple) is the largest
17.
The Larynx
• Epiglottis
⚬Spoon-shapedflap of elastic cartilage
⚬Protects the superior opening of the larynx
⚬Routes food to the posteriorly situated esophagus and
routes air toward the trachea
⚬During swallowing, the epiglottis rises and forms a lid
over the opening of the larynx
18.
The Larynx
• Vocalfolds (true vocal cords)
⚬Vibrate with expelled air
⚬Allow us to speak
• The glottis includes the vocal cords and the
opening between the vocal cords
19.
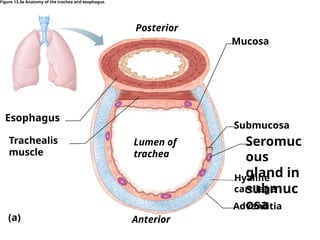
The Trachea
• Commonlycalled the windpipe
• 4-inch-long tube that connects to the larynx
• Walls are reinforced with C-shaped rings of
hyaline cartilage, which keep the trachea patent
(open)
• Lined with ciliated mucosa
⚬Cilia beat continuously in the opposite direction of
incoming air
⚬Expel mucus loaded with dust and other debris away
from lungs
The Main Bronchi
•Formed by division of the trachea
• Each bronchus enters the lung at the hilum
(medial depression)
• Right bronchus is wider, shorter, and straighter
than left
• Bronchi subdivide into smaller and smaller
branches
23.
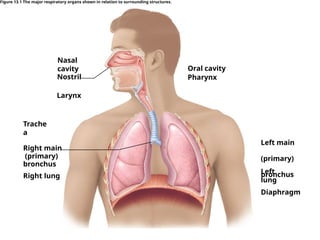
Figure 13.1 Themajor respiratory organs shown in relation to surrounding structures.
Nasal
cavity
Trache
a
Right main
(primary)
bronchus
Left main
(primary)
bronchus
Nostril
Oral cavity
Pharynx
Larynx
Right lung
Diaphragm
Left
lung
24.
The Lungs
• Occupythe entire thoracic cavity except for the
central mediastinum
• Apex of each lung is near the clavicle (superior
portion)
• Base rests on the diaphragm
• Each lung is divided into lobes by fissures
⚬Left lung—two lobes
⚬Right lung—three lobes
25.
The Lungs
• Serosacovers the outer surface of the lungs
⚬Pulmonary (visceral) pleura covers the lung surface
⚬Parietal pleura lines the walls of the thoracic cavity
• Pleural fluid fills the area between layers
⚬Allows the lungs to glide over the thorax
⚬Decreases friction during breathing
• Pleural space (between the layers) is more of a
potential space
26.
The Lungs
• Thebronchial tree
⚬Main bronchi subdivide into smaller and smaller
branches
⚬Bronchial (respiratory) tree is the network of branching
passageways
⚬All but the smallest passageways have reinforcing
cartilage in the walls
⚬Conduits to and from the respiratory zone
⚬Bronchioles (smallest conducting passageways)
27.
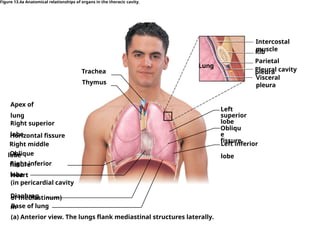
Figure 13.4a Anatomicalrelationships of organs in the thoracic cavity.
Visceral
pleura
Rib
Pleural cavity
Left
superior
lobe
Left inferior
lobe
Obliqu
e
fissure
Thymus
Trachea
Apex of
lung
Right superior
lobe
Horizontal fissure
Oblique
fissure
Right middle
lobe
Right inferior
lobe
Heart
(in pericardial cavity
of mediastinum)
Diaphrag
m
Base of lung
Lung
Parietal
pleura
(a) Anterior view. The lungs flank mediastinal structures laterally.
Intercostal
muscle
28.
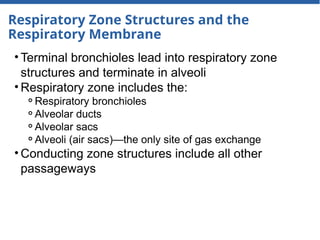
Respiratory Zone Structuresand the
Respiratory Membrane
• Terminal bronchioles lead into respiratory zone
structures and terminate in alveoli
• Respiratory zone includes the:
⚬Respiratory bronchioles
⚬Alveolar ducts
⚬Alveolar sacs
⚬Alveoli (air sacs)—the only site of gas exchange
• Conducting zone structures include all other
passageways
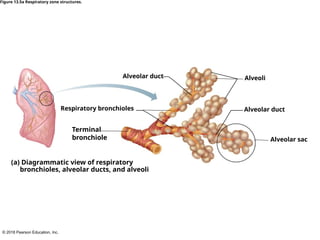
Alveolar
pores
Alveolus
(b) Light micrographof human lung tissue, showing
the final divisions of the respiratory tree (120×)
Alveolar
duct
Figure 13.5b Respiratory zone structures.
31.
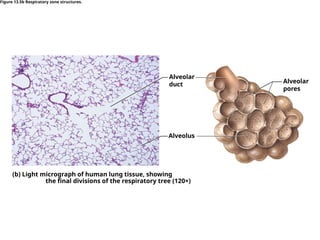
Respiratory Zone Structuresand the
Respiratory Membrane
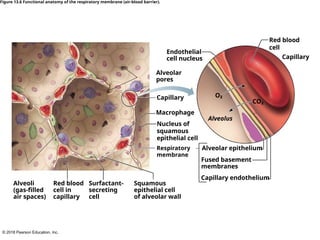
• Alveoli
⚬Simple squamous epithelial cells largely compose the
walls
⚬Alveolar pores connect neighboring air sacs
• Pulmonary capillaries cover external surfaces of
alveoli
32.
Respiratory Zone Structuresand the
Respiratory Membrane
• Respiratory membrane (air-blood barrier)
⚬On one side of the membrane is air, and on the other
side is blood flowing past
⚬Formed by alveolar and capillary walls
• Gas crosses the respiratory membrane by
diffusion
⚬Oxygen enters the blood
⚬Carbon dioxide enters the alveoli
The Gas ExchangeProcess
• Oxygen intake: When you inhale, oxygen-rich air
enters the lungs and reaches the alveoli.
• Diffusion: Oxygen diffuses through the thin walls
of the alveoli into the surrounding capillaries,
where it binds to red blood cells.
36.
The Gas ExchangeProcess
• Carbon dioxide removal: At the same time,
carbon dioxide, a waste product of cellular
metabolism, diffuses out of the capillaries and
into the alveoli.
• Exhalation: When you exhale, the carbon
dioxide-rich air is expelled from the lungs.
37.
Respiratory Physiology
• Functionsof the respiratory system
⚬Supply the body with oxygen
⚬Dispose of carbon dioxide
• Respiration includes four distinct events
(discussed next)
⚬Pulmonary ventilation
⚬External respiration
⚬Respiratory gas transport
⚬Internal respiration
38.
Respiratory Physiology
• Fourevents of respiration
1.Pulmonary ventilation—moving air into and out of the
lungs (commonly called breathing)
2.External respiration—gas exchange between
pulmonary blood and alveoli
■ Oxygen is loaded into the blood
■ Carbon dioxide is unloaded from the blood
39.
Respiratory Physiology
• Fourevents of respiration (continued)
1.Respiratory gas transport—transport of oxygen and
carbon dioxide via the bloodstream
2.Internal respiration—gas exchange between blood and
tissue cells in systemic capillaries
40.
Mechanics of Breathing
•Pulmonary ventilation
⚬Mechanical process that depends on volume changes
in the thoracic cavity
⚬Volume changes lead to pressure changes, which lead
to the flow of gases to equalize pressure
41.
Mechanics of Breathing
•Two phases of pulmonary ventilation
⚬Inspiration = inhalation
■ Flow of air into lungs
⚬Expiration = exhalation
■ Air leaving lungs
42.
Mechanics of Breathing
•Inspiration (inhalation)
⚬Diaphragm and external intercostal muscles contract
⚬Intrapulmonary volume increases
⚬Gas pressure decreases
⚬Air flows into the lungs until intrapulmonary pressure
equals atmospheric pressure
43.
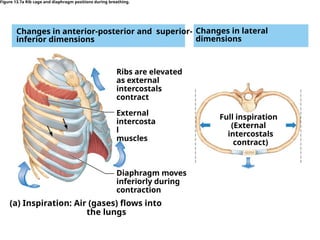
(a) Inspiration: Air(gases) flows into
the lungs
Changes in lateral
dimensions
Changes in anterior-posterior and superior-
inferior dimensions
Figure 13.7a Rib cage and diaphragm positions during breathing.
Ribs are elevated
as external
intercostals
contract
External
intercosta
l
muscles
Diaphragm moves
inferiorly during
contraction
Full inspiration
(External
intercostals
contract)
44.
Mechanics of Breathing
•Expiration (exhalation)
⚬Largely a passive process that depends on natural lung
elasticity
⚬Intrapulmonary volume decreases
⚬Gas pressure increases
⚬Gases passively flow out to equalize the pressure
⚬Forced expiration can occur mostly by contraction of
internal intercostal muscles to depress the rib cage
45.
Mechanics of Breathing
•Intrapleural pressure
⚬The pressure within the pleural space) is always
negative
⚬Major factor preventing lung collapse
⚬If intrapleural pressure equals atmospheric pressure,
the lungs recoil and collapse
46.
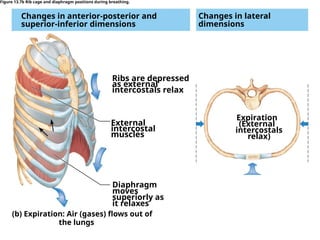
Ribs are depressed
asexternal
intercostals relax
(b) Expiration: Air (gases) flows out of
the lungs
External
intercostal
muscles
Diaphragm
moves
superiorly as
it relaxes
Changes in lateral
dimensions
Changes in anterior-posterior and
superior-inferior dimensions
Figure 13.7b Rib cage and diaphragm positions during breathing.
Expiration
(External
intercostals
relax)
47.
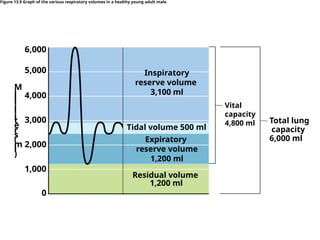
Respiratory Volumes andCapacities
• Factors affecting respiratory capacity
⚬Size
⚬Sex
⚬Age
⚬Physical condition
• Tidal volume (TV)
⚬Normal quiet breathing
⚬500 ml of air is moved in/out of lungs with each breath
48.
Respiratory Volumes andCapacities
• Inspiratory reserve volume (IRV)
⚬Amount of air that can be taken in forcibly over the tidal
volume
⚬Usually around 3,100 ml
• Expiratory reserve volume (ERV)
⚬Amount of air that can be forcibly exhaled after a tidal
expiration
⚬Approximately 1,200 ml
49.
Respiratory Volumes andCapacities
• Residual volume
⚬Air remaining in lung after expiration
⚬Cannot be voluntarily exhaled
⚬Allows gas exchange to go on continuously, even
between breaths, and helps keep alveoli open (inflated)
⚬About 1,200 ml
50.
Respiratory Volumes andCapacities
• Vital capacity
⚬The total amount of exchangeable air
⚬Vital capacity = TV + IRV + ERV
⚬4,800 ml in men; 3,100 ml in women
• Dead space volume
⚬Air that remains in conducting zone and never reaches
alveoli
⚬About 150 ml
51.
Respiratory Volumes andCapacities
• Functional volume
⚬Air that actually reaches the respiratory zone
⚬Usually about 350 ml
• Respiratory capacities are measured with a
spirometer
52.
Vital
capacity
4,800 ml Totallung
capacity
6,000 ml
Inspiratory
reserve volume
3,100 ml
Tidal volume 500 ml
Expiratory
reserve volume
1,200 ml
Residual volume
1,200 ml
M
i
l
l
i
l
i
t
e
r
s
(
m
l
)
1,000
2,000
3,000
4,000
5,000
6,000
0
Figure 13.9 Graph of the various respiratory volumes in a healthy young adult male.
53.
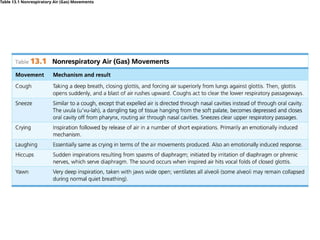
Nonrespiratory Air Movements
•Can be caused by reflexes or voluntary actions
• Examples
⚬Cough and sneeze—clears lungs of debris
⚬Crying—emotionally induced mechanism
⚬Laughing—similar to crying
⚬Hiccup—sudden inspirations
⚬Yawn—very deep inspiration
Respiratory Sounds
• Soundsare monitored with a stethoscope
• Two recognizable sounds can be heard with a
stethoscope:
1.Bronchial sounds—produced by air rushing through
large passageways such as the trachea and bronchi
2.Vesicular breathing sounds—soft sounds of air filling
alveoli
56.
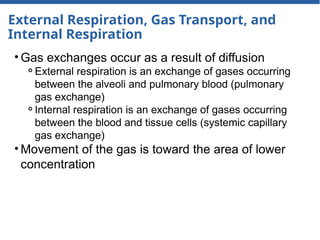
External Respiration, GasTransport, and
Internal Respiration
• Gas exchanges occur as a result of diffusion
⚬External respiration is an exchange of gases occurring
between the alveoli and pulmonary blood (pulmonary
gas exchange)
⚬Internal respiration is an exchange of gases occurring
between the blood and tissue cells (systemic capillary
gas exchange)
• Movement of the gas is toward the area of lower
concentration
External Respiration
• Oxygenis loaded into the blood
⚬Oxygen diffuses from the oxygen-rich air of the alveoli
to the oxygen-poor blood of the pulmonary capillaries
• Carbon dioxide is unloaded out of the blood
⚬Carbon dioxide diffuses from the blood of the
pulmonary capillaries to the alveoli
59.
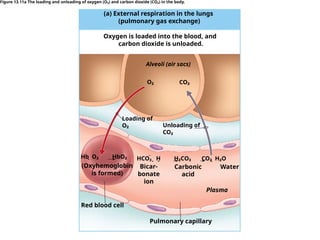
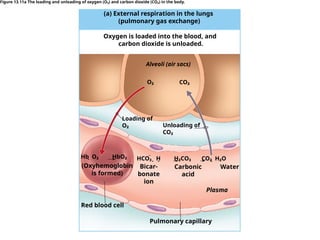
(a) External respirationin the lungs
(pulmonary gas exchange)
Oxygen is loaded into the blood, and
carbon dioxide is unloaded.
Alveoli (air sacs)
O₂ CO₂
Loading of
O₂ Unloading of
CO₂
Hb O₂ HbO₂
HCO₃ H H₂CO₃ CO₂ H₂O
(Oxyhemoglobin
is formed)
Bicar-
bonate
ion
Carbonic
acid
Water
Red blood cell
Pulmonary capillary
Plasma
Figure 13.11a The loading and unloading of oxygen (O₂) and carbon dioxide (CO₂) in the body.
60.
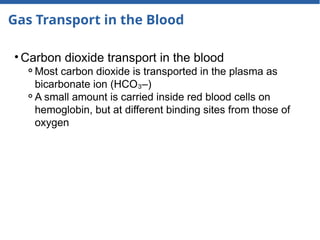
Gas Transport inthe Blood
• Oxygen transport in the blood
⚬Most oxygen travels attached to hemoglobin and forms
oxyhemoglobin (HbO )
₂
⚬A small dissolved amount is carried in the plasma
61.
(a) External respirationin the lungs
(pulmonary gas exchange)
Oxygen is loaded into the blood, and
carbon dioxide is unloaded.
Alveoli (air sacs)
O₂ CO₂
Loading of
O₂ Unloading of
CO₂
Hb O₂ HbO₂
HCO₃ H H₂CO₃ CO₂ H₂O
(Oxyhemoglobin
is formed)
Bicar-
bonate
ion
Carbonic
acid
Water
Red blood cell
Pulmonary capillary
Plasma
Figure 13.11a The loading and unloading of oxygen (O₂) and carbon dioxide (CO₂) in the body.
62.
Gas Transport inthe Blood
• Carbon dioxide transport in the blood
⚬Most carbon dioxide is transported in the plasma as
bicarbonate ion (HCO –)
₃
⚬A small amount is carried inside red blood cells on
hemoglobin, but at different binding sites from those of
oxygen
63.
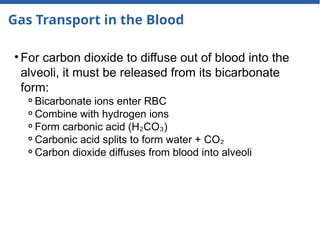
Gas Transport inthe Blood
• For carbon dioxide to diffuse out of blood into the
alveoli, it must be released from its bicarbonate
form:
⚬Bicarbonate ions enter RBC
⚬Combine with hydrogen ions
⚬Form carbonic acid (H CO )
₂ ₃
⚬Carbonic acid splits to form water + CO₂
⚬Carbon dioxide diffuses from blood into alveoli
64.
(a) External respirationin the lungs
(pulmonary gas exchange)
Oxygen is loaded into the blood, and
carbon dioxide is unloaded.
Alveoli (air sacs)
O₂ CO₂
Loading of
O₂ Unloading of
CO₂
Hb O₂ HbO₂
HCO₃ H H₂CO₃ CO₂ H₂O
(Oxyhemoglobin
is formed)
Bicar-
bonate
ion
Carbonic
acid
Water
Red blood cell
Pulmonary capillary
Plasma
Figure 13.11a The loading and unloading of oxygen (O₂) and carbon dioxide (CO₂) in the body.
65.
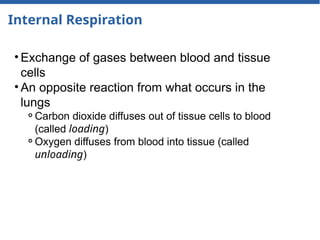
Internal Respiration
• Exchangeof gases between blood and tissue
cells
• An opposite reaction from what occurs in the
lungs
⚬Carbon dioxide diffuses out of tissue cells to blood
(called loading)
⚬Oxygen diffuses from blood into tissue (called
unloading)
66.
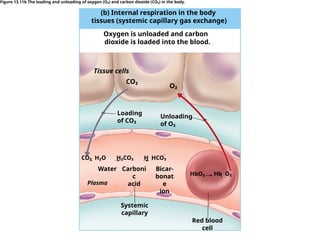
(b) Internal respirationin the body
tissues (systemic capillary gas exchange)
Oxygen is unloaded and carbon
dioxide is loaded into the blood.
Tissue cells
CO₂
O₂
Unloading
of O₂
Loading
of CO₂
HbO₂ Hb O₂
Water Bicar-
bonat
e
ion
Systemic
capillary
Red blood
cell
Carboni
c
acid
CO₂ H₂O H₂CO₃ H HCO₃
Plasma
Figure 13.11b The loading and unloading of oxygen (O₂) and carbon dioxide (CO₂) in the body.
67.
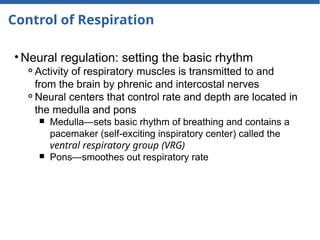
Control of Respiration
•Neural regulation: setting the basic rhythm
⚬Activity of respiratory muscles is transmitted to and
from the brain by phrenic and intercostal nerves
⚬Neural centers that control rate and depth are located in
the medulla and pons
■ Medulla—sets basic rhythm of breathing and contains a
pacemaker (self-exciting inspiratory center) called the
ventral respiratory group (VRG)
■ Pons—smoothes out respiratory rate
68.
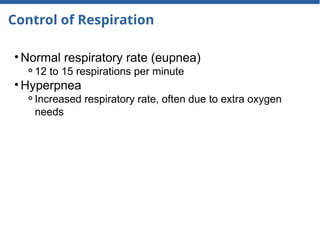
Control of Respiration
•Normal respiratory rate (eupnea)
⚬12 to 15 respirations per minute
• Hyperpnea
⚬Increased respiratory rate, often due to extra oxygen
needs
69.
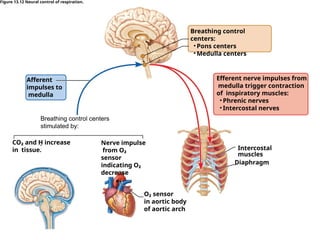
Breathing control
centers:
• Ponscenters
• Medulla centers
Breathing control centers
stimulated by:
O₂ sensor
in aortic body
of aortic arch
Intercostal
muscles
CO₂ and H increase
in tissue.
Nerve impulse
from O₂
sensor
indicating O₂
decrease
Afferent
impulses to
medulla
Efferent nerve impulses from
medulla trigger contraction
of inspiratory muscles:
• Phrenic nerves
• Intercostal nerves
Figure 13.12 Neural control of respiration.
Diaphragm
70.
Control of Respiration
•Non-neural factors influencing respiratory rate and
depth
⚬Physical factors
■ Increased body temperature
■ Exercise
■ Talking
■ Coughing
⚬Volition (conscious control)
⚬Emotional factors such as fear, anger, and excitement
71.
Control of Respiration
•Non-neural factors influencing respiratory rate and
depth (continued)
⚬Chemical factors: CO levels
₂
■ The body’s need to rid itself of CO is the
₂ most important
stimulus for breathing
■ Increased levels of carbon dioxide (and thus, a
decreased or acidic pH) in the blood increase the rate
and depth of breathing
■ Changes in carbon dioxide act directly on the medulla
oblongata
72.
Control of Respiration
•Non-neural factors influencing respiratory rate and
depth (continued)
⚬Chemical factors: oxygen levels
■ Changes in oxygen concentration in the blood are
detected by chemoreceptors in the aorta and common
carotid artery
■ Information is sent to the medulla
■ Oxygen is the stimulus for those whose systems have
become accustomed to high levels of carbon dioxide as a
result of disease
73.
Control of Respiration
•Non-neural factors influencing respiratory rate and
depth (continued)
⚬Chemical factors (continued)
■ Hyperventilation
• Rising levels of CO in the blood (acidosis) result in faster,
₂
deeper breathing
• Exhale more CO to elevate blood pH
₂
• May result in apnea and dizziness and lead to alkalosis
74.
Control of Respiration
•Non-neural factors influencing respiratory rate and
depth (continued)
⚬Chemical factors (continued)
■ Hypoventilation
• Results when blood becomes alkaline (alkalosis)
• Extremely slow or shallow breathing
• Allows CO to accumulate in the blood
₂
75.
Developmental Aspects ofthe Respiratory
System
• Lungs do not fully inflate until 2 weeks after birth
⚬This change from nonfunctional to functional respiration
depends on surfactant
⚬Surfactant lowers surface tension so the alveoli do not
collapse
⚬Surfactant is formed late in pregnancy, around 28 to 30
weeks
76.
Developmental Aspects ofthe Respiratory
System
• Respiratory rate changes throughout life
⚬Newborns: 40 to 80 respirations per minute
⚬Infants: 30 respirations per minute
⚬Age 5: 25 respirations per minute
⚬Adults: 12 to 18 respirations per minute
⚬Rate often increases again in old age
77.
Developmental Aspects ofthe Respiratory
System
• Asthma
⚬Chronically inflamed, hypersensitive bronchiole
passages
⚬Respond to irritants with dyspnea, coughing, and
wheezing
78.
Developmental Aspects ofthe Respiratory
System
• Youth and middle age
⚬Most respiratory system problems are a result of
external factors, such as infections and substances that
physically block respiratory passageways
79.
Developmental Aspects ofthe Respiratory
System
• Aging effects
⚬Elasticity of lungs decreases
⚬Vital capacity decreases
⚬Blood oxygen levels decrease
⚬Stimulating effects of carbon dioxide decrease
⚬Elderly are often hypoxic and exhibit sleep apnea
⚬More risks of respiratory tract infection







![L12__Respiratory_system_anatomy[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/l12respiratorysystemanatomy1-230531143920-02738076-thumbnail.jpg?width=640&height=640&fit=bounds)