Download to read offline




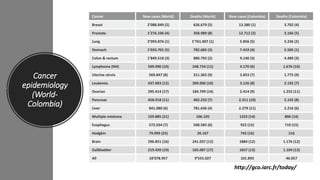
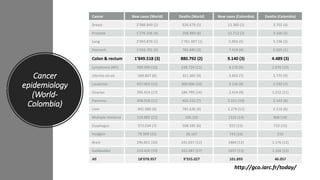
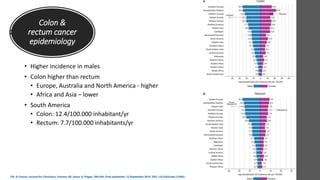
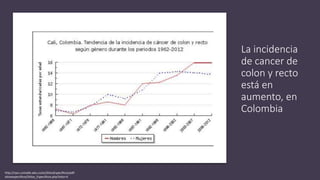
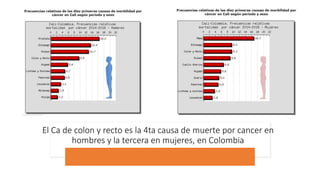
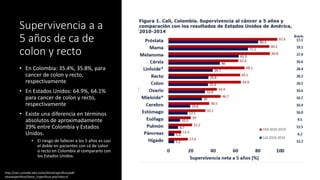

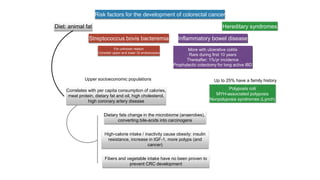


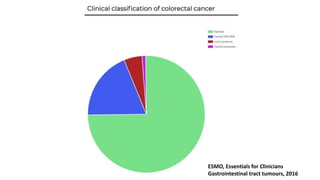
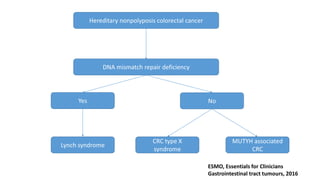
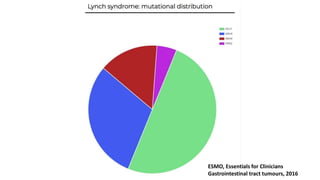

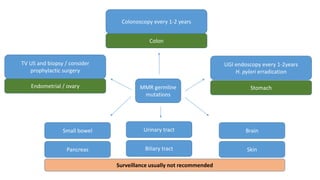
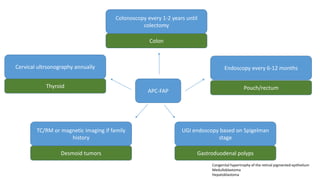
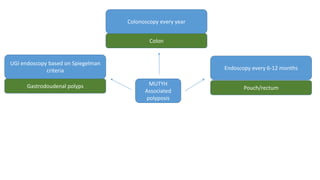
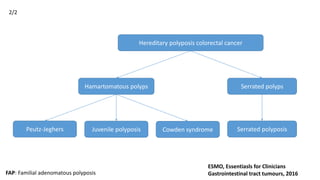
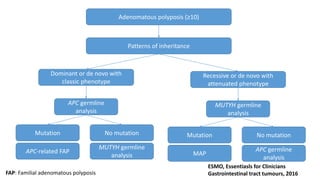
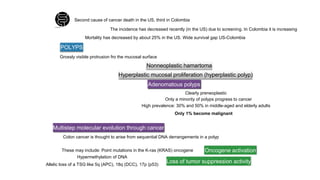
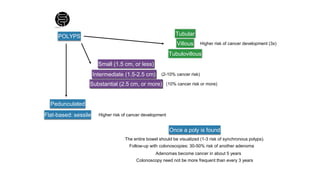

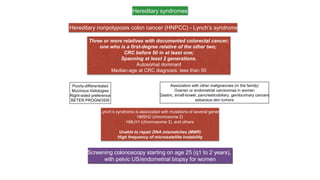

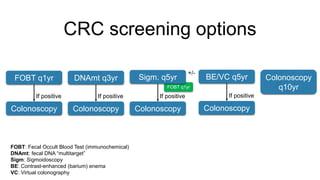
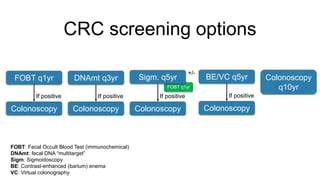












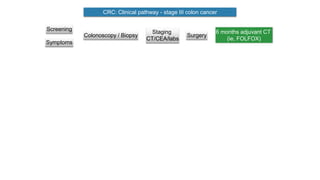
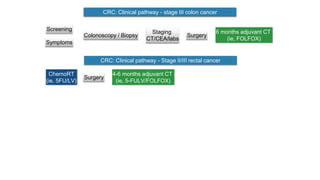
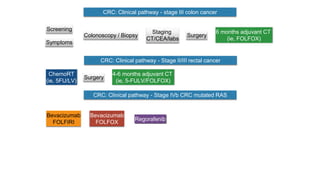
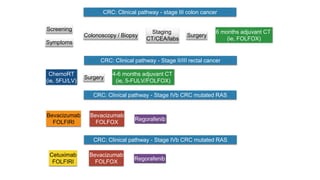
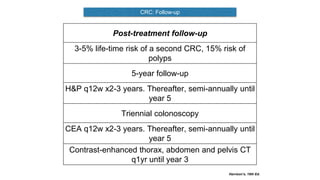
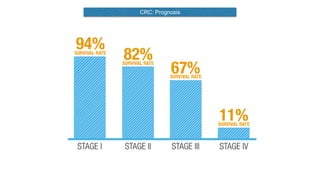

This document provides information about colorectal cancer, including: - Colorectal cancer is the third leading cause of cancer death in Colombia. Survival rates are much lower in Colombia than the US. - Risk factors include diet high in fat and low in fiber, obesity, inflammatory bowel disease, family history, and hereditary syndromes. - Hereditary syndromes associated with colorectal cancer include Lynch syndrome, familial adenomatous polyposis (FAP), and MUTYH-associated polyposis (MAP). - Diagnosis involves screening via colonoscopy to detect polyps which can be removed to prevent cancer development. Staging determines cancer extent and guides treatment.





































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















