Downloaded 40 times


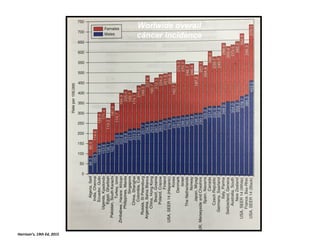




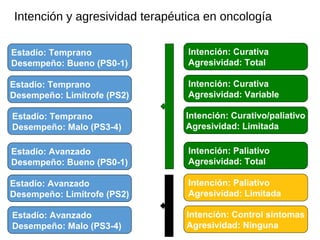


This document provides an overview of an oncology course for medical students. It discusses that cancer is curable in almost 2/3 of patients but is a catastrophic event for the patient and their family. It changes a person's self-image and how they are viewed by others. The document also covers cancer statistics worldwide, common causes, screening and diagnosis, staging, treatment intent and aggressiveness based on stage and performance status, and supportive care including management of symptoms like pain, depression, and nausea.