The document discusses the anatomy of fascial spaces in the head and neck region. It describes several layers of deep cervical fascia including the investing layer, middle layer, visceral layer, vertebral layer and alar fascia. It also outlines the boundaries and contents of various fascial spaces such as the buccal space, retropharyngeal space, submandibular space and submental space. Clinical aspects such as drainage of abscesses in these spaces are also mentioned.





















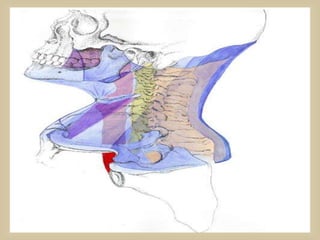







![ BOUNDARIES
Anteroinferiorly : anterior belly of digastric
Posteroinferiorly : posterior belly of
digastric
Superiorly or base : base of the mandible
and the line joining the angle of the
mandible and mastoid process
CONTENT
Submandibular gland; submandibular lymph
nodes; hypoglossal nerve [XII]; mylohyoid
nerve; facial artery and vein](https://image.slidesharecdn.com/neckspaceanatomy-171103185849/85/Neck-space-anatomy-31-320.jpg)



![ Tributaries to common facial vein
Cervical branch of facial nerve[VII]
Common carotid artery
External and internal carotid arteries
Superiorthyroid; ascending pharyngeal; lingual, facial, and occipital arteries
Internal jugular vein
Vagus [X], accessory [XI],and hypoglossal [XII] nerves
Superiorand inferior roots of ansa cervicalis
Transverse cervical nerve](https://image.slidesharecdn.com/neckspaceanatomy-171103185849/85/Neck-space-anatomy-35-320.jpg)































































































































































