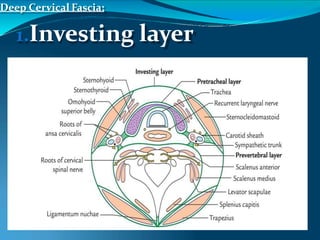
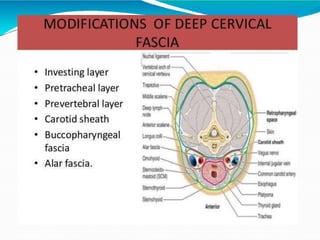
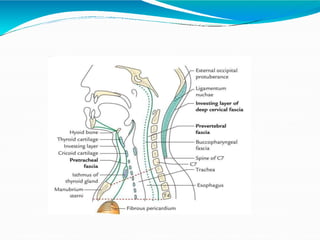
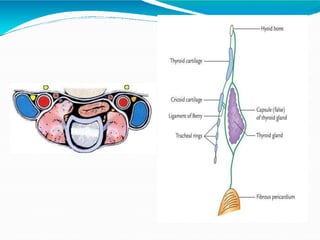
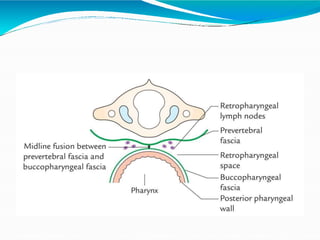
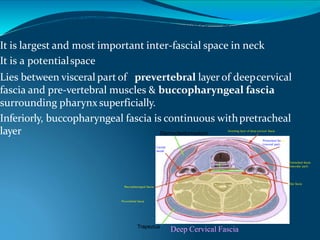
The document discusses the deep fascia of the neck, which compartmentalizes the structures in the neck into four major fascial compartments. The deep fascia consists of three layers - the investing layer, pretracheal layer, and prevertebral layer. The investing layer surrounds the neck, while the pretracheal layer encloses the infrahyoid muscles, thyroid gland, trachea, and esophagus. The prevertebral layer forms a sheath for the vertebral column and associated deep cervical muscles. Between these layers are the neurovascular compartments containing the carotid arteries, internal jugular veins, vagus nerves and deep cervical lymph nodes.