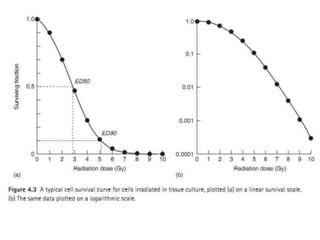
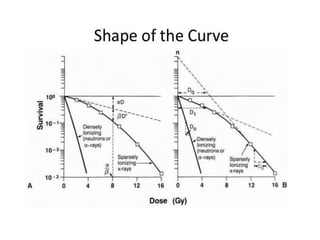
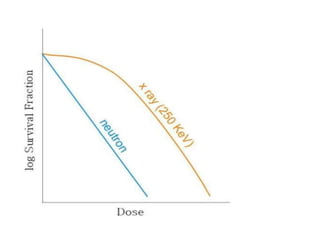
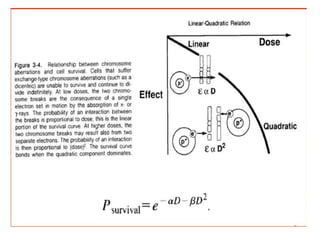
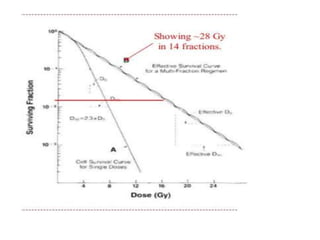
Cell survival curves show the relationship between radiation dose and the proportion of cells that survive. For low linear energy transfer (LET) radiation like X-rays, the curve starts with a shoulder region followed by an exponential decrease in survival fraction. The linear-quadratic model describes cell survival as an exponential function of dose, with parameters α and β representing linear and quadratic components of cell killing. Fractionation reduces cell survival more than single high doses by allowing repair of sublethal damage between fractions. Hypoxic cells are less sensitive initially but may reoxygenate and become sensitive to later fractions. Mitotic cell death is the most common mode of radiation-induced cell death in tumor cells.
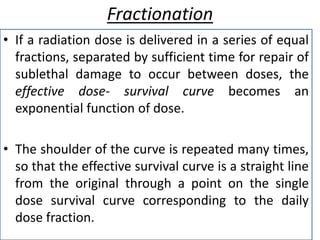
![Multitarget theory
• According to this theory, some cells contain more
than one target and each of this targets should
receive the hit.
• The curve starts with less sensitive region at low
dose and tend to become exponential at larger
doses. So they present a shoulder at small doses.
• Here the SF is given by the equation:
S = 1- [1-exp(-D/nD˳)]ⁿ
Where n is the no of targets in the organisms.](https://image.slidesharecdn.com/cellsurvivalcurveppt-170917183154/85/Cell-survival-curve-ppt-16-320.jpg)
























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












