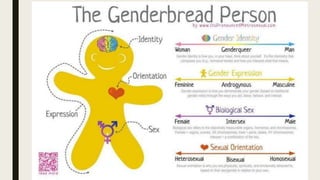
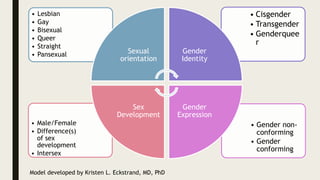
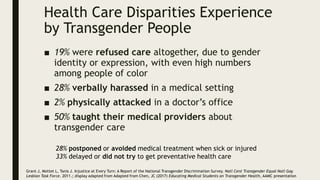
This document provides an overview of a symposium on culturally effective care for LGBT populations. It begins with an agenda that includes differentiating key terms, defining intersectionality, identifying health disparities and social determinants of health, and applying concepts through a case study. The document then defines various terms related to gender identity, sexual orientation, sex, and development. It reviews the history of pathologization of LGBT identities in medicine and mental health. Statistics on demographics and health disparities experienced by LGBT populations are presented. Strategies for providing culturally effective care include creating an inclusive environment, building trust, ensuring confidentiality, and using inclusive language. Local and national resources for LGBT care are also listed.




































































![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)




