
Download as PDF, PPTX
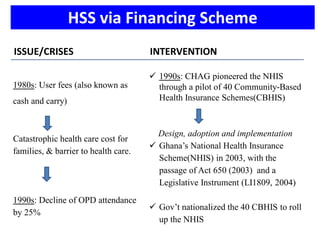
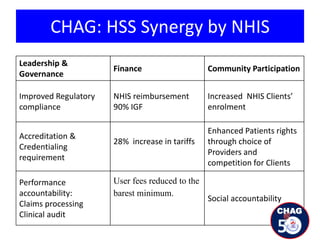

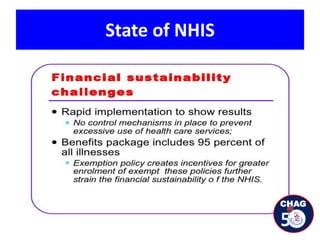






The document discusses the role of the Christian Health Association of Ghana (CHAG) in enhancing health systems resilience in Ghana, emphasizing its collaborative relationship with the government since its establishment in 1967. It highlights CHAG's contributions to health financing, achievements through the National Health Insurance Scheme, challenges faced, and lessons learned to improve health service delivery and sustainability. The take-home message stresses the importance of partnerships and advocacy for achieving Universal Health Coverage (UHC).























































































