Download to read offline


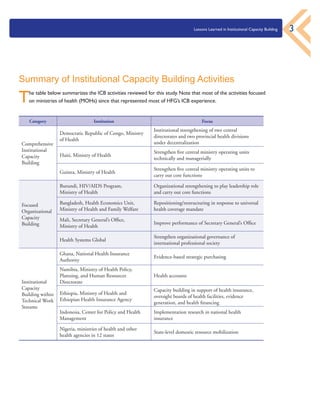














The document discusses lessons learned from the Health Finance and Governance (HFG) project's efforts in institutional capacity building (ICB) since 2012, highlighting the necessity of building sustainable health system capacities. It identifies key areas for successful ICB, including taking a systems perspective, engaging senior leadership, conducting thorough diagnostics, and the importance of skilled personnel in implementation. Ultimately, these lessons aim to guide future health systems strengthening initiatives to improve governance and expand universal health coverage.























































































