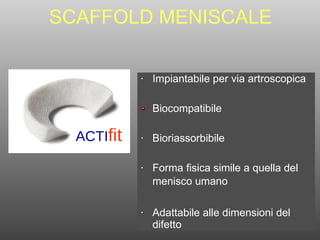
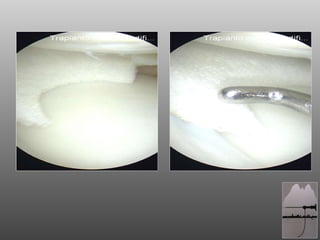
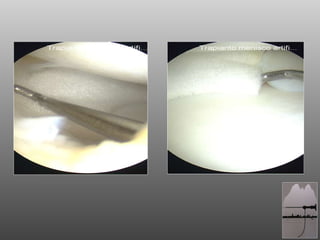
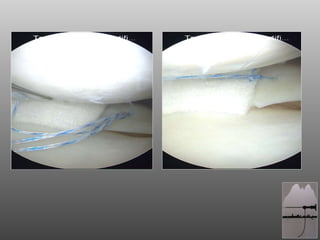
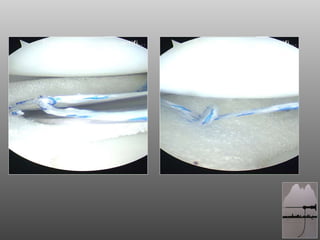
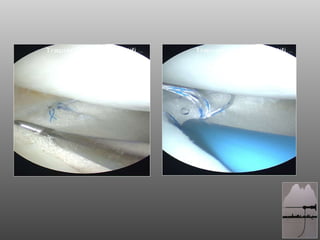
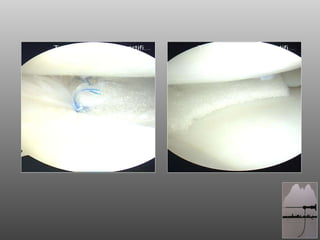
Il documento discute un caso clinico relativo all'uso di uno scaffold meniscale per il trattamento di lesioni meniscali, evidenziando la superiorità delle tecniche di riparazione rispetto alla meniscectomia totale. Viene descritto un nuovo impianto biocompatibile e bioriassorbibile, progettato per facilitare la crescita cellulare e per essere adattabile alle dimensioni del difetto. Conclude sottolineando l'importanza di salvaguardare il menisco e la necessità di una selezione accurata dei pazienti e di tecniche chirurgiche appropriate.







![GRAZIE [email_address]](https://image.slidesharecdn.com/casoclinicoactifit1-101005073507-phpapp02/85/Caso-clinico-actifit-1-22-320.jpg)

































