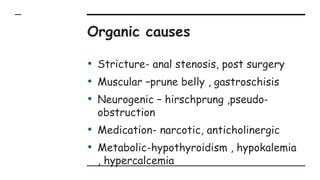
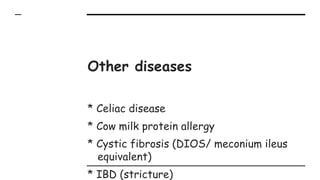
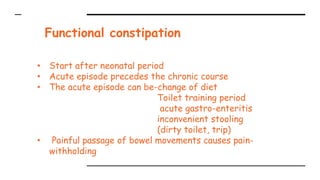
Tanya is a 4-year-old girl presenting with a 2-year history of constipation, opening her bowels every 5 days and straining with intermittent abdominal pain and occasional soiling. A hard stool mass is palpable on examination. Constipation can be caused by organic issues like strictures or functional issues like withholding behavior after painful bowel movements. Treatment involves softening the stool with laxatives, relieving impaction, patient education on diet and toilet habits, and behavioral management.


































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




